

37 years old lady presenting with long standing history of hip problems. She had problems related to bilateral hip dysplasia ever since childhood and was told that both her hips were out of place. In her early thirties she had left hip replacement which did not completely relieve her pains. She had several episodes of dislocation for which she needed to be first put in a spica case for sometimes followed by prolonged wearing of abduction braces. She presented to us with bilateral hip pains though her right side was the most troublesome.
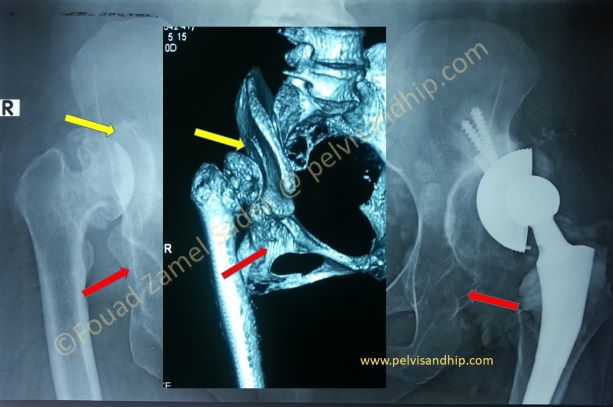
On this plain AP view of the pelvis one can see clearly the right dislocated Type III dislocation. The acetabulum has never been occupied by the femoral head which is articulating with a false acetabulum. The left total hip replacement is far from ideal. The cup has been inserted in the false acetabulum and although vertical, the head is still in the liner. Having been able to walk on it for the previous 3 years you may argue that there is some osteointegration in the superolateral part of the cup with the superolateral false acetabulum. Both acetabulae are still virgins with neither cup nor femoral head in them. The 3D CT (in the middle) is very clear for the right hip with a false acetabulum (yellow arrows), below the true acetabulum is empty (red arrow)
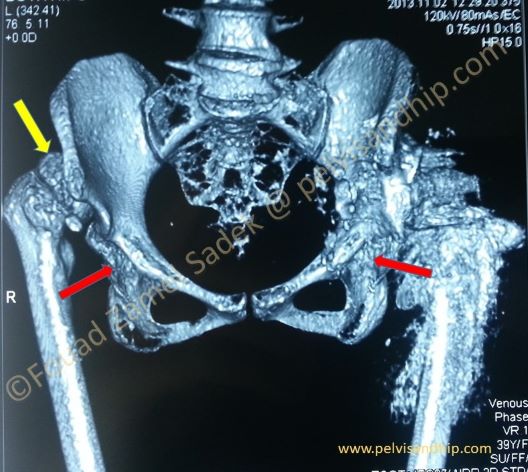
3D reconstruction CT showing an anterior view of the pelvis. The right hip is clearly dislocated articulating with the false acetabulum (yellow arrow); with the true acetabulum empty. The left hip shows a lot of distorting metal artifacts from the prosthesis nevertheless still showing clearly the empty true acetabulum (red arrow)
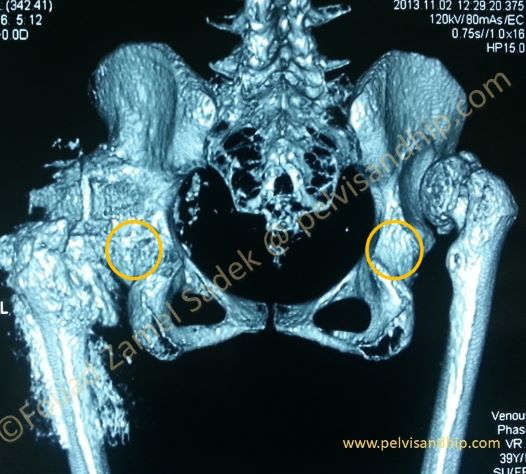
A posterior view of the 3D CT of the pelvis. The rings shows where by the true acetabulum is and on the right side you can easily appreciate the more inviting and easier to reach false acetabulum once one approaches these hips and follows the space where the femoral head was residing, a common mistake for the non-wary surgeon which would lead to a false high placement of the acetabular during replacement. In these cases, the surgeon has to search inferiorly for the true acetabulum which usually looks obliterated as seen by the following axial CT cuts.
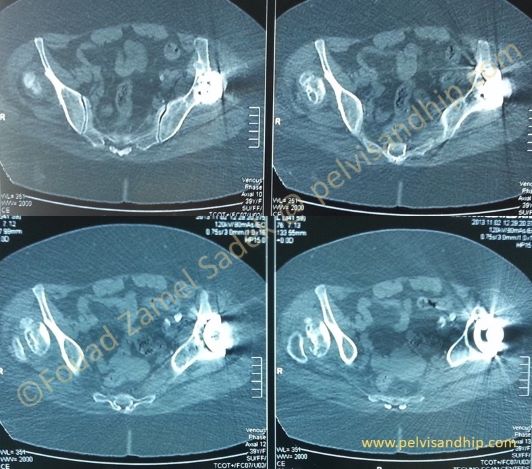
One of the best ways of carrying out a detailed study of the dysplastic hip is to have a sequential study of all the axial cuts of the CT examination from proximal to distal. This examination allows the surgeon to form a very clear understanding of the status of the acetabulum he/she is dealing with. Superiorly, the supraacetabulum (false) is not offering the best bone stock as is clear on the left hip where the cup was wrongly placed.
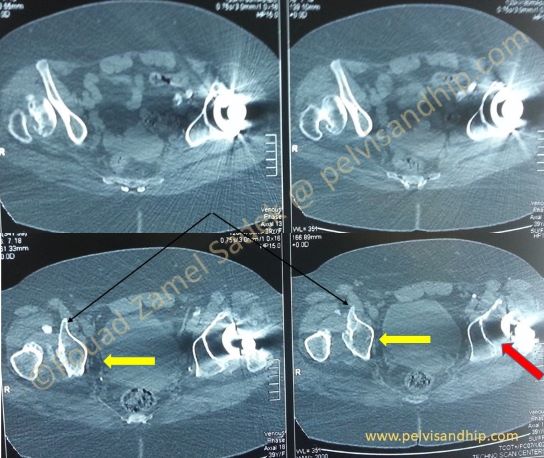
Proceeding more distally you can appreciate the best bone stock which is very clear on the right hip distally to the anterior inferior iliac spines (two black arrows); the dome of the acetabulum which will offer the best bone support can be clearly identified (yellow arrow). On the left hip the most inferior part of the replaced cup barely reaches the true acetabulum (red arrow)

Going more and more distally, on both sides the acetabulum is untouched and offers the best bone stock. You can notice the significantly underdeveloped walls both anterior and posterior. During reaming to carve the acetabulum to take a cup, bone is usually very soft and it helps one to appreciate the real depth of each acetabulum in order not perforate the floor which the surgeon can have an idea about by drilling the floor and measuring the depth. The acetabulum is very similar to a horse saddle and the cavity is filled with tissue admixed immature bone islands.

The best site of placement of the cup is where the true acetabulum is with the best bone stock as can be seen more interestingly on the left hip which was previously replaced in this case.
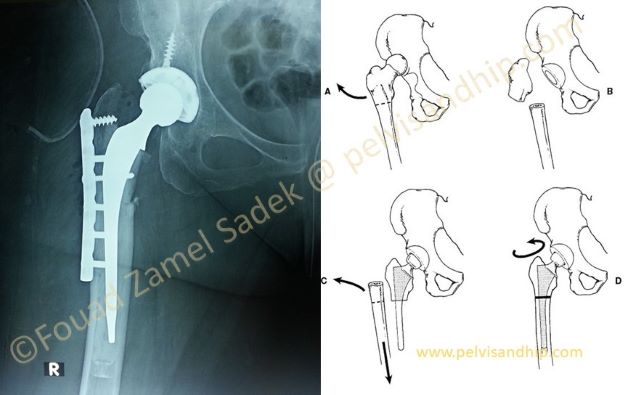
Based on the techniques published in the J. of Arthroplasty, 4:351, 1988, by Sonseller P, and Mc Beath A, describing as shown on the diagram the technique of shortening osteotomy during a high dislocation replacement in a case dysplasia, we inserted this hypbrid hip. A subtrochanteric shortening femoral osteotomy was done and fixed with this narrow DCP with insertion of a cemented stem. The cup was inserted in the true acetabulum; notice that a standard 46mm cup was used with no need for special implant.
The leg length was changed by elongating the recently replaced right hip bringing the center of rotation at the ICR of the native hip.
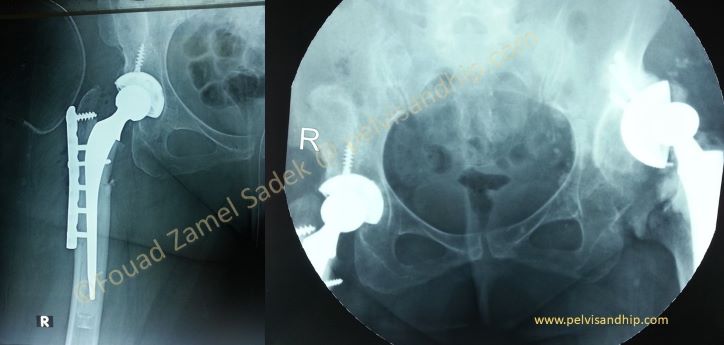
Once our patient started to walk the left hip was dislocated. In the dislocated position you can notice that the cup empty of the pushing head has settled back in the false acetabulum; clearly showing that the cup has been loose with no osteointegration. The plan now was to place the cup in the anatomical true acetabulum and revise the left hip.

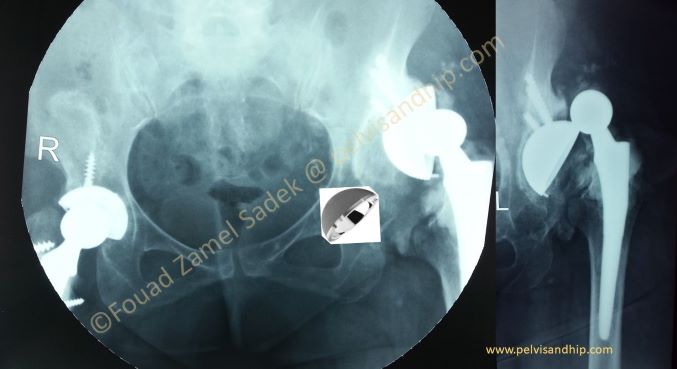
The left hip was revised with removal of the loose cup and insertion of a new one in the true acetabulum and insertion of another cement on cement stem. In the left hip there was no need to do any femoral osteotomies.
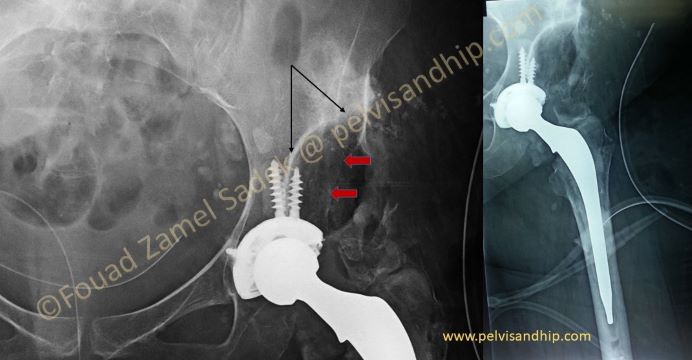
The thick while curve line (black arrows) of the false acetabulum gives a false impression that the cup is not covered with good bone stock. The two red arrows show the faint edge of the ilium covering the dome of the acetabulum with good bone stock for the cup.

The learning points: 1.Replacing a total hip in a dysplastic hip especially with high dislocation is challenging and requires good understanding of the pathological anatomy. 2.The aim is to place the acetabular component in the true acetabulum avoiding first a high hip center and a false acetabulum implantation. 3.Good acetabular exposure ensures adequate replacement. 4.Remember that the true acetabulum is not only underdeveloped, but it is also oval in shape, extremely soft with underdeveloped walls but offers the best bone stock for the acetabular component implantation, which in most times with adequate preparation is a standard implant. 5.Subtrochanteric femoral shortening osteotomy is a good technique to bring down the femur to its anatomical position and also to protect the sciatic nerve from a stretch injury.

If you feel like posting comments, enquiries or questions please click here.