

48 years male presented with pain after having a total hip replacement done in 2006. Presented to us in 2008 walking with crutches. There was a history of previous trauma to the left hip 20 years earlier. In 2006 he had severe hip pain for which he had this replacement. He was told that this was a cementless cup with a ceramic on ceramic for longevity. He says that he started touch weight bearing with crutches 2 months after the index surgery, with pain ever since the replacement that increases with any activity.

Analysis of the clinical findings reveals pain in the hip region with a feeling of instability. The pain is activity related with a characteristic starting pain with walking. There is pain on rotation in bed. Examination shows that he is only able to walk with a stick due to pain. There is pain around the thigh with passive rotation associated with thigh tenderness. Such findings draw our attention that the origin of this patient’s pain is probably coming from the femoral stem.

Our patient shows us two previous CRP assessments one in 2007 with a value of 36 and a second one 7 months later in 2008 with a CRP of 21 and an ESR of 28/57. Although these values cannot elucidate our diagnosis with confirmation or exclusion of infection, our next step was to carry out a combined Technitium 99 with Gallium 67 scan. Report of this disclaimed an active linear Ga 67 avid uptake at the left femoral shaft corresponding to overperfused active Tc 99mm MDP uptake, referring to active inflammation. The only valuable information is that the source pain is probably from around the femur but not conclusive about its nature.

Through a posterolateral approach the following findings were identified. The operative field was dry with no effusion. The cup was very stable. There was a metal head used on top of a seemingly stable stem with no obvious toggling. Hammering on the stem, attempting extraction, had no effect on the stem.
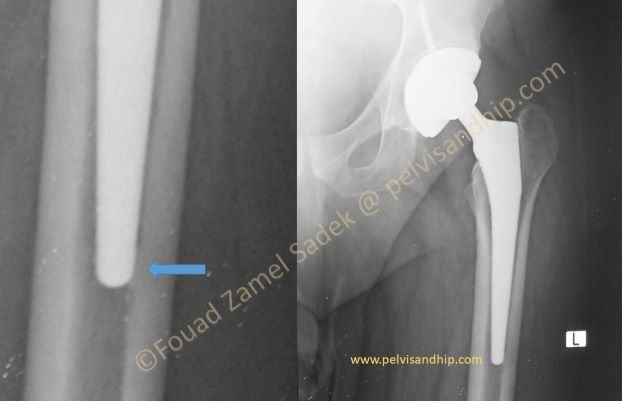
A closer look to the tip of the femur revealed this osteoingetraion at the tip of the stem what may be regarded like an incomplete attempt at pedestal formation (arrow) something that can drive one’s suspicion about the presence of a minimally toggling stem due to lack of adequate osteointegration in the proximal part of the stem with only integration distally. Such a finding represent an explanation to the pain and a prediction to a significant difficulty of loosening the stem for endofemoral revision.

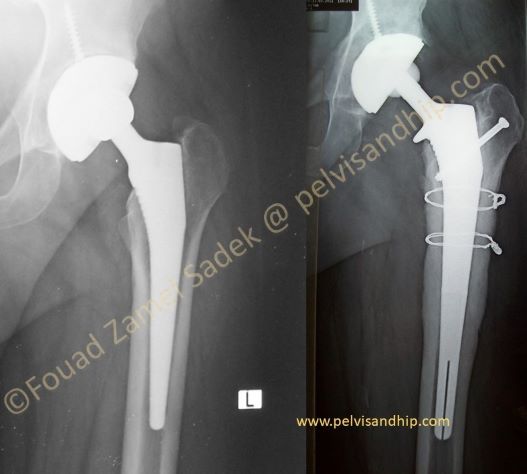
The choice was to perform an extended trochanteric osteotomy which is a controlled explosion rather than an uncontrolled one. This allowed a well executed removal of the stem with repair of the osteotomy with revision with a longer cementless stem (long corail previously known as Le Carr). A ceramic head was added to the stem. The cup was left untouched.

Follow up at 6 months after healing of the osteotomy and well after perfect osteointegration of the stem. The patient walks normally with no pain and no limp.

Leg length is equalized. The previously inserted cup was in somewhat a more vertical position than the standard but is causing no effect on the hip function or stability.
Learning points: 1.A painful total hip is not an expected finding after a successful implantation by contrast to a total knee. 2.History of the previous surgery is the first step to analyze a painful total hip implantation. 3.Careful analysis of the pain includes it occurrence; starting pain is an indication of some lack of stability probably in the stem. Groin pain is indicative of hip origin. Pain with rotation and turning over in bed as well as tenderness of the thigh are all sign of stem problems. 4.Radiological signs looked for include radiolucent lines, spot welding and pedestal formation. 5.An extended trochanteric osteotomy is the best to explant a well integrated or even a resistant stem to explantation.

If you feel like posting comments, enquiries or questions please click here.