

30 years old war victim who presented one year after a neglected transverse with posterior wall fracture. Associated posterior hip dislocation; by contrast to the usual central dislocation of most transverse fractures. He has 5cm shortening with an adduction deformity of the right thigh. He is walking with a single leg gait using crutches as his right foot does not reach the ground.
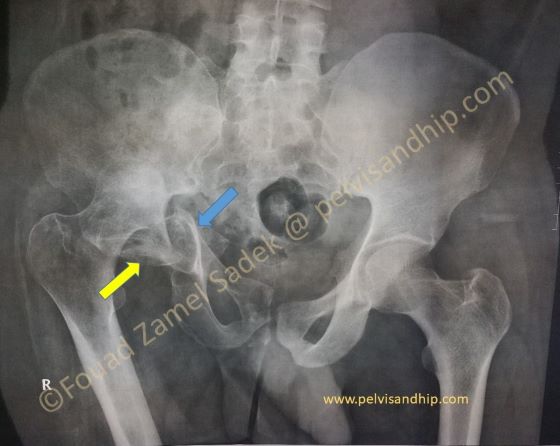
AP view of the pelvis with an associated pelvic and acetabular fracture; associated transverse with posterior wall. The one year injury precludes any attempt at hip preservation. Nevertheless for a total hip implantation there are different obstacles. The distal hemipelvis is significantly medially displaced (blue arrow) leaving no remaining actetabular walls or columns to anchor a cup on. The posterior wall is inside the dome (yellow arrow). The high femoral head from the neglected dislocation will also represent difficulties in bringing down the hip to the center of rotation. The following radiological studies show these obstacles.
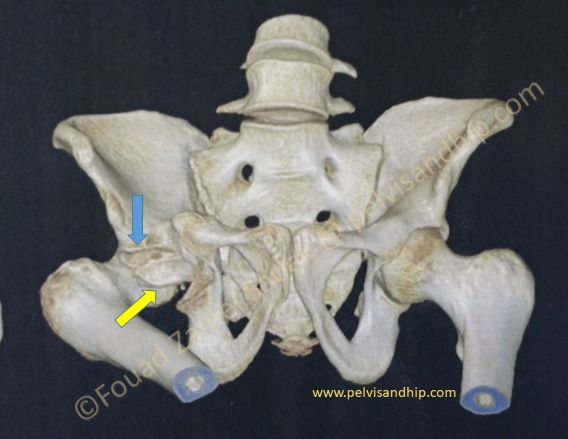
On the 3D reconstruction one can appreciate the remaining dome (blue arrow) with no distal walls or columns; these have migrated medially and need to be brought back to the lateral anatomical position. The posterior wall is inside the dome (yellow arrow). The right hip is obviously in fixed flexion and adduction.

Note the damaged femoral head (blue arrow). The medial position of the hemipelvis with it the walls and columns of the acetabulum (yellow arrow). The posterior wall is clear residing in the dome (red arrow).
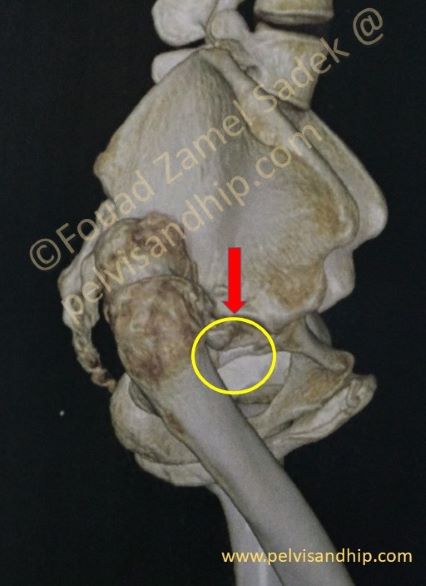
On this lateral view of the 3D reconstruction one can appreciate the postero-superior position of the hip (femoral head). The dome appears clearly (red arrow) with an empty space (yellow circle) distal to it whereby it would be very difficulty to insert a cup with conventional techniques of reconstruction. This is a case for delayed osteotomy of the transverse fracture, reduction and fixation aiming to allow a total hip implantation.
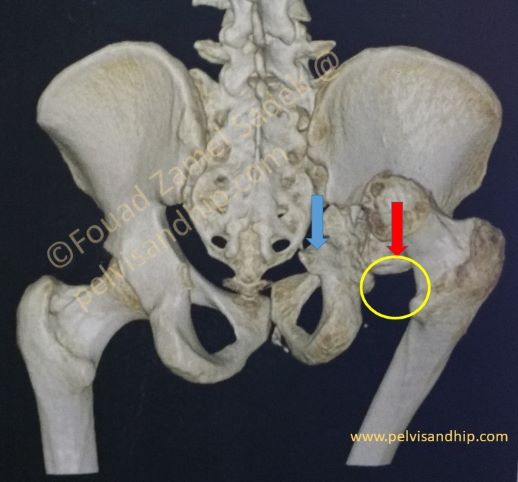
On this posterior view of the pelvis the relationship of the remaining dome (red arrow) to the medially displaced column with the distal hemipelvis (blue arrow) is very obvious. The supposed site of the cup (yellow circle) is quite clear.

The surgical plan: 1. floppy lateral position for access both anteriorly and posteriorly. In the semi supine position we do first a symphyseal osteotomy. 2. A classic ilioinguinal approach is done to osteotomize the anterior column part of the transverse fracture. 3. Through a posterior approach the femoral head is resected followed by posterior releases and posterior column osteotomies.
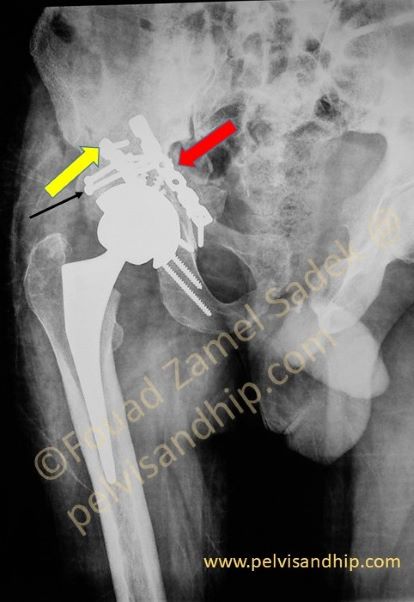
After the first 3 steps in preparation; the transverse fracture is mobilized after releasing the sacrospinous and sacrotuberous ligaments. The transverse fracture is well fixed with both an anterior (red arrow) and a posterior (yellow arrow) plates. Femoral autografting was done to fill the posterior wall fracture defect and fixed with 2 standard screws (black arrow) A standard cementless cup is placed with a cross-linked poly and a ceramic head with an HA coated cementless stem. There was no need to do any femoral osteotomies.

This immediate postoperative pelvic view shows the restoration of the center of rotation and leg length.

The two main technical issues about the delayed mobilization of a neglected posterior column fracture is first to release the sacrospinous ligament (red arrow) which is preferable done by osteotomy of the base of the pelvic spine. When this is released together with the scarring of the fracture plane, the whole posterior column can be slightly twisted to make it easier to dissect the sciatic nerve (yellow arrow) and reach the sacro-tuberous ligament (blue arrow). Once this is released the mobilization of the posterior column becomes complete and simple.

Learning points:
Some significant defects resulting from acetabular fractures require special studies out of scope of the classical classifications of acetabular defects for total hip implantation.
Delayed reduction and fixation of the acetabular fractures may be needed for restoration of the bone stock and reproducing the center of rotation of the hip.
A combined floppy lateral position is very useful and less traumatic than extensile approaches.
With associated pelvis injuries (in this case the symphysis disruption); this should be dealt with first before mobilizing the acetabular fracture.
Adequate releases of the sacrospinous and sacrotuberous ligament are an integral part of the posterior mobilization, without which mobilization becomes very difficult.
A step by step carefully carried out procedure will lead us to the desired end result; implantation of a standard prosthesis in the anatomical center of rotation for a well functioning hip.

If you feel like posting comments, enquiries or questions please click here.