
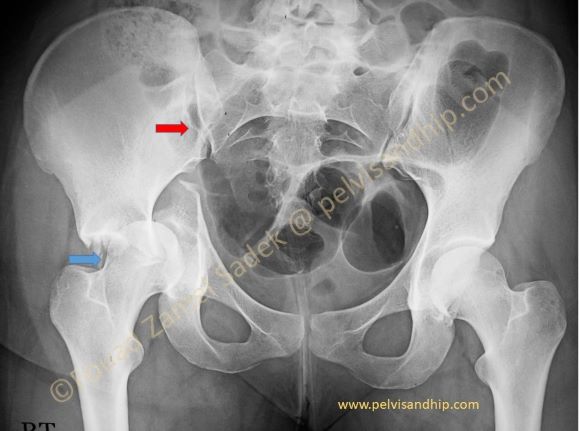
AP view of the pelvis in a 20 years old young lady who had an RTA that caused acetabular fracture of the right hip. On this pelvic view we can see a transverse fracture associated with what looks like a posterior wall (blue arrow). Associated widening of the ipsilateral right SI joint (red arrow) is commonly observed in transverse fractures associated with a central dislocation of the femoral head probably due to wedging of the head in the fracture gap pushing the distal hemipelvis medially and the proximal ilium laterally opening the SI joint.

The outlet view of the pelvis shows the widening of the right SI joint much more clearly. In this view the intact ischiopubic ramus is one of the easy signs to differentiate between, a T fracture where the latter tends to be fractured, and a transverse fracture as in this case. The central femoral head dislocation is one of the risk factors for damage to the cartilage of the femoral head which tends to be scaffolded by the sharp fractured bone.

The iliac oblique view shows the transverse fracture with a low posterior column and as seen in the next picture with a high anterior column. In this young age group the reduction of the transverse fracture becomes very critical for a satisfactory result. Note the very low fracture of the posterior column in this view (arrow)
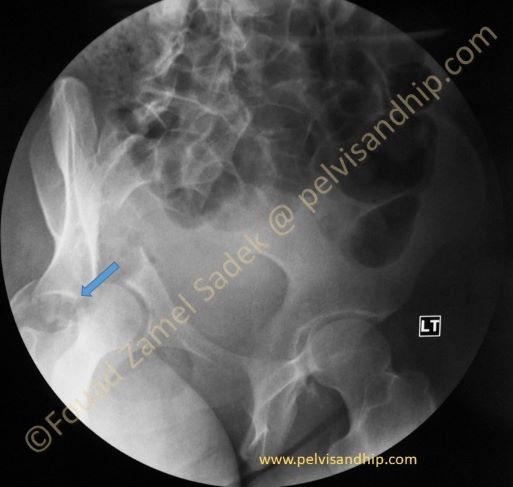
The iliac oblique view confirms the transtectal nature of this fracture. Wedging of the femoral head puts it at risk (arrow). The posterior wall fracture is clear. The very high anterior component of the transverse fracture would be very difficult to reduce anatomically from a posterior approach. Letournel used to choose an extensile approach for the anatomical reduction of a transtectal fracture. The plan is to use a combined approach with an ilioinguinal one first for reduction and fixation of the transverse fracture followed by a posterior approach.
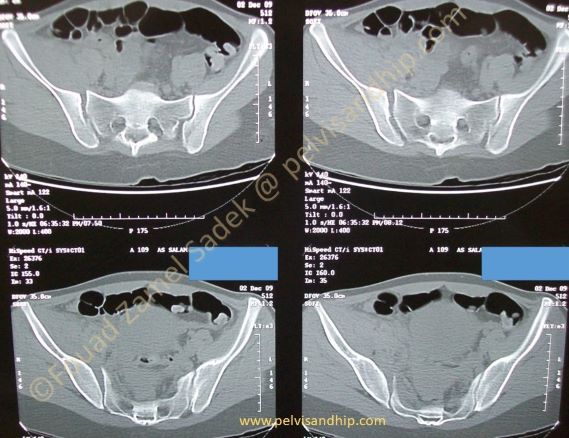
This axial CT view shows clearly the widening of the right SI joint by comparison to the left SI joint. This is not an associated pelvic fracture but the isolated SI joint injury caused by the wedged femoral head in the fracture plane.
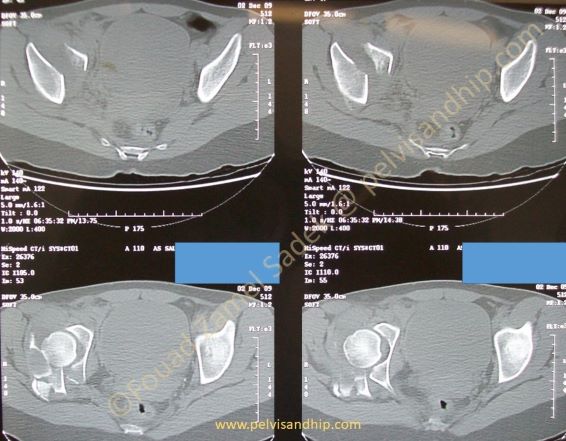
The distal CT cuts show clearly the high transverse fracture of the acetabulum associated with the comminuted posterior wall.

This so-called section 6 of the axial CT scan which tends to go through the dome of the acetabulum shows that the transverse fracture is quite high and is in deed a transtectal fracture.

The 3D CT reconstruction is very informative showing the wide SI joint mentioned earlier, the wedged femoral head into the fracture plane, the orientation of the transverse fracture as well as the posterior wall fracture. All data can be comprehensively accumulated from all views staring with the plain x-rays and ending up with all available views of the CT study of the injury.

The inlet view although not one of the classic views needed for an acetabular fracture, (this is here shown on the 3D reconstruction), this views sows clearly the pattern of displacement that we usually see with any transverse fracture with rotation of the distal hemipelvis around 2 planes and 2 axises.
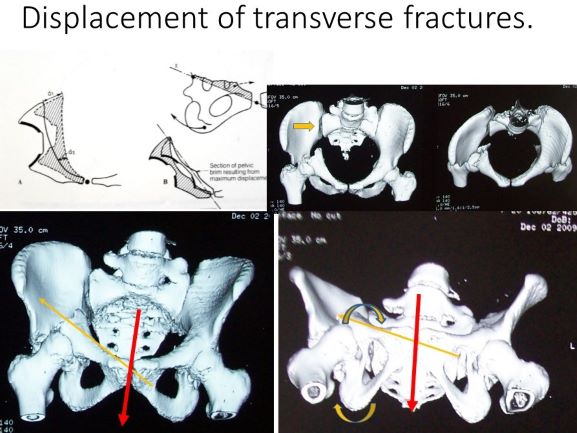
Displacement occurs along two axes. The first (thin yellow arrow) going from the symphysis to the middle of the fracture plane; this axis is directed from anteriorly and medially to posteriorly slightly upwards and laterally. The fractured segment rotates around this axis with the pubic ramus superiorly tilting inwards and the ischial tuberosity inferiorly tilts outwards. The second axis is a vertical one along the front plane of the pelvis, through the symphysis; the hemipelvis rotates around this axis inwards like a door with its hinges along that axis (thick red arrow)
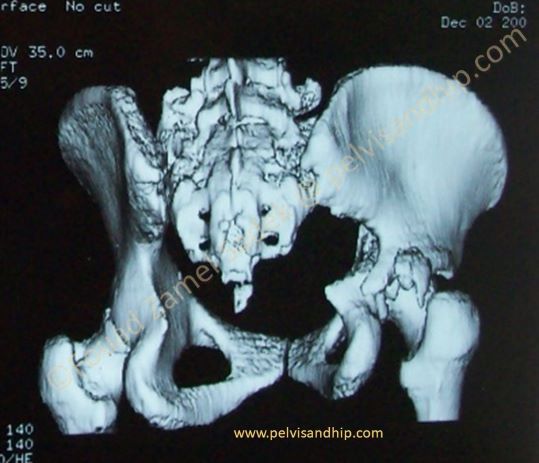
This posterior view of the 3D reconstruction of the pelvis clearly shows the comminuted associated posterior wall fracture as well as the low fracture of the posterior column.

Obturator oblique view on intraoperative fluoroscopy, shows the anterior fixation with a long reconstruction plate done as the first stage of the surgical reconstruction. The posterior wall is quite obvious on this view (arrow). The widened more posterior end of the transverse fracture would be closed through the posterior approach by another posterior plate for both the transverse fracture as well as the posterior wall.
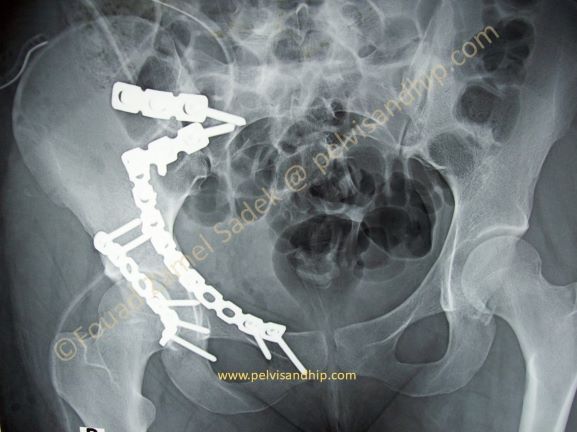
AP view of the full reconstruction showing 3 steps of fixation; first the closure of the SI joint with plate fixation (an SI screw could have been used instead). Second the anterior plate for the high anterior column fractured and thirdly the posterior plate for the posterior wall as well as the posterior column.
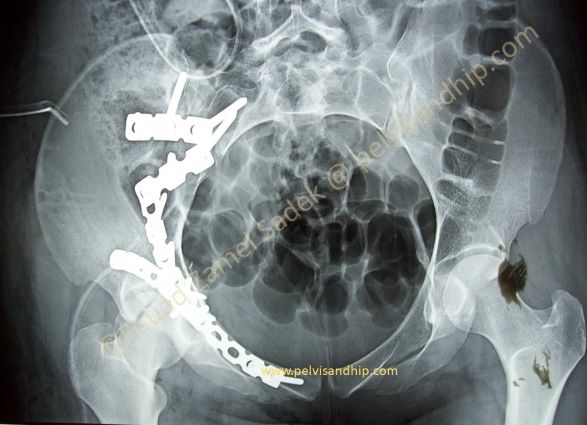
This rather uncommon view in this injury was chosen just to appreciate the global reconstruction of the pelvis and the acetabulum and to appreciate the position of the anterior plate along the brim and its relation to the anterior SI plates.

The learning points from this case: 1.Appreciate all the components of a complex injury of this associated transverse with posterior wall fracture. 2.Note the associated widening of the SI joint which is common with a central head dislocation. 3.Sometimes, despite an associated posterior wall fracture the choice of the first surgical approach was an anterior approach for the anatomical reduction of the transverse fracture (in this case a transtectal fracture which needs special attention). 4.Meticulous step by step planning is more mandatory in complex injuries to obtain the satisfactory results aimed at. This young lady was reviewed after 10 years with a normally functional hip.

If you feel like posting comments, enquiries or questions please click here.