

45 years old male with a neglected posterior column fracture. Hip has been dislocated for more than 8 weeks. Options of delayed reconstruction with hip preservation was considered initially but with preparation for total hip replacement as well.

Iliac oblique view shows the significantly displaced posterior column with the obvious damage of the femoral head (arrow) which make us choose a total hip replacement with acetabular reconstruction. A large segmental posterior defect is anticipated. This is what we call a single column defect that would need a delayed osteotomy of the posterior column for acetabular reconstruction.
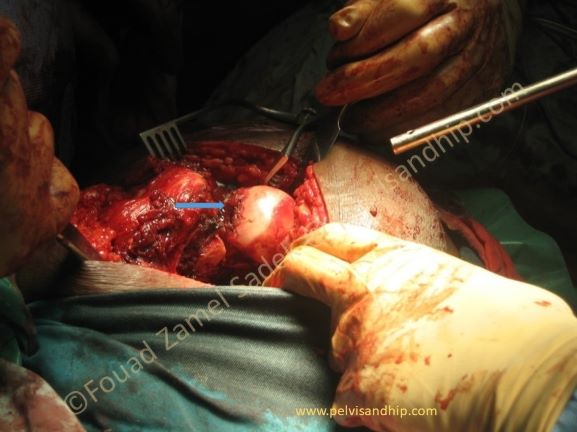
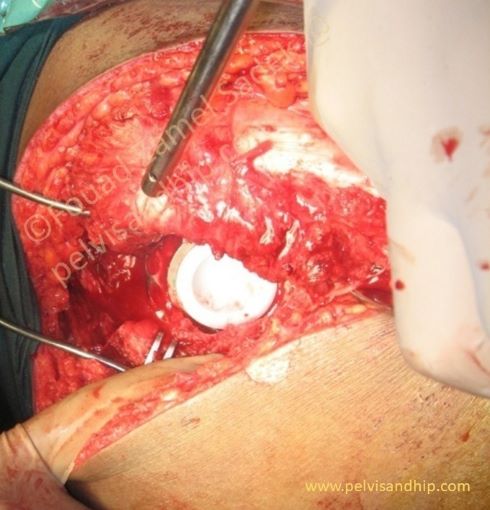
Through a posterior approach the femoral head is dislocated and the head damage is obvious. The approach in this case is more similar to the Kocker-Langenbeck approach for acetabular reconstruction than the standard posterolateral approach for total hip implantation.
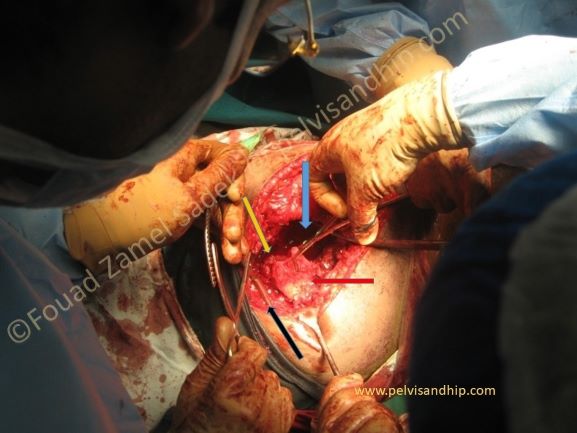
After resection of the femoral head, the acetabulum (blue arrow) was identified and cleared of the soft tissue. The exposed posterior column was held with a clamp by the assistant (red arrow). After clearing the fracture (yellow arrow), a pointed reduction clamp is inserted with one arm into the lesser sciatic notch (black arrow) and the other arm in the supraacetabular area for reduction of the posterior column.

The pelvic reduction clamp was closed by the surgeon and the posterior column was mobilized and manipulated into closing the defect of the fracture. Reduction is not anatomical which is not the aim in such cases. The aim is to prepare the acetabulum to be fit for accepting a press fit cementless cup after reaming.
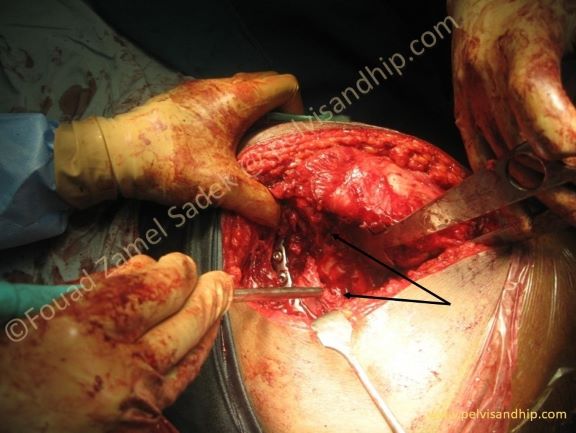
A 3.5 reconstruction plate was applied to the posterior column to fix the fracture and the acetabulum has been brought back to its sphericity (arrows) with no defect that would jeopardize the stability of the cup.
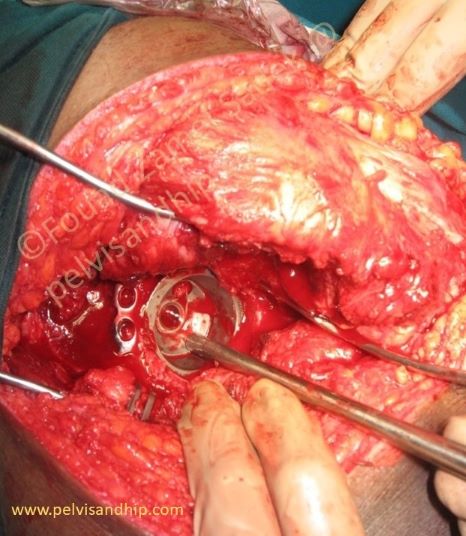
After reaming a cementless porous coated cup was inserted and found to be stable as a press fit cup with no initial screws. These were added for extra stability.
The polyethylene was inserted and a ceramic head was used to improve longevity of the prosthesis.
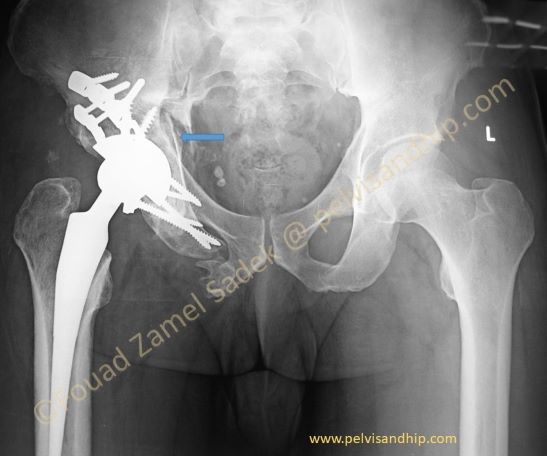
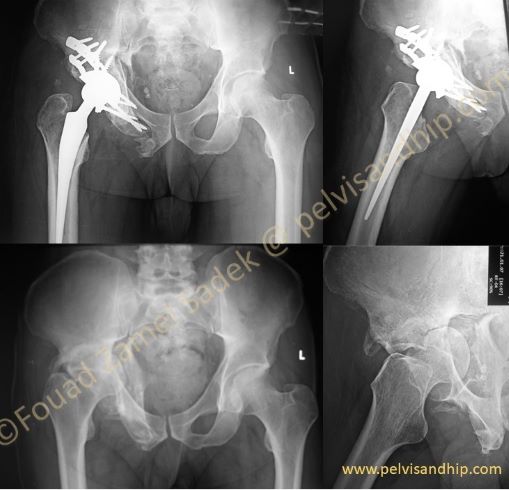
Postoperative x-rays shows the cementless reconstruction with 2 plates inserted for the stability of the posterior column. One can appreciated the posterior column mobilization (arrow) from its previously displaced position obliterating the acetabular defect. If there is an another posterior wall defect the femoral head can sometimes be used as an extra source of autografting.

The lateral view of the hip reconstruction with better viewing of the posterior column in this rather iliac oblique projection.
The points of learning: 1.Delayed reconstruction of an acetabular fracture should never be attempted without a total hip preparation on the side. 2.Some post acetabular fractures are better reconstructed with delayed osteotomies for acetabular reconstructions to take a cementless cup. Among these the displaced single column fractures 3.An anatomical reduction is not mandatory as the aim is to close the acetabular defect and reaming would prepare the acetabulum to its sphericity. 4.For cementless cup implantation, press fit stability should be obtained and screw addition should only be optional. 5.Better weight bearing options; ceramic/cross-linked poly has become the first choice for younger active patients.

If you feel like posting comments, enquiries or questions please click here.