
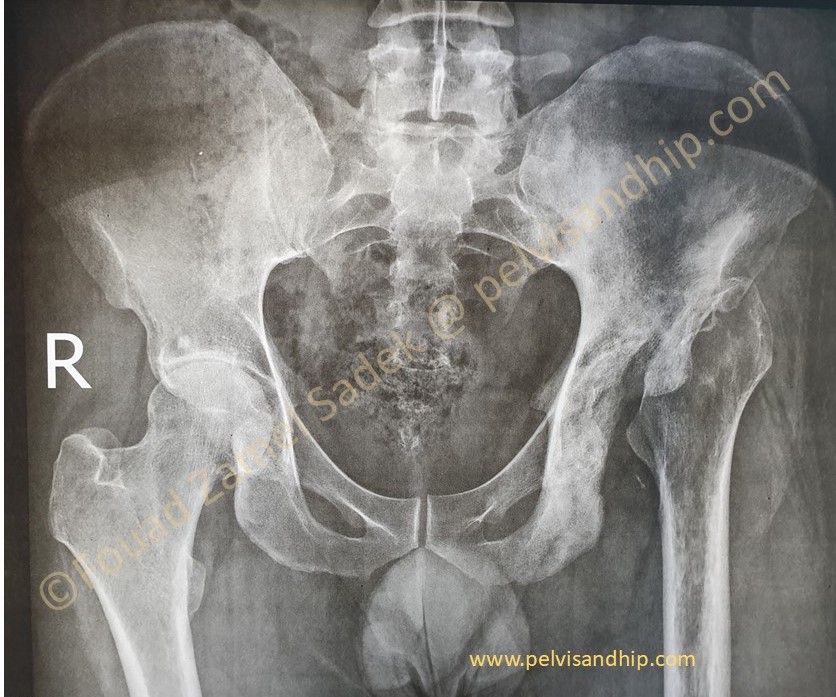
A 34 years old male with a two years history of previous infections related to the left hip and pelvis. Previous surgical interventions to clear infection carried out more than a year ago with no obvious recurrence of infective related issues. Note that he also has arthritic changes on the right hip as well.
At presentation, clinically infection was cleared and inflammatory profiles are all normal. Patient coming asking to have a joint replacement for better function and improvement of quality of life. He is only able to mobilize with crutches and foot can barely touch the ground. He is not able to work in his current status.
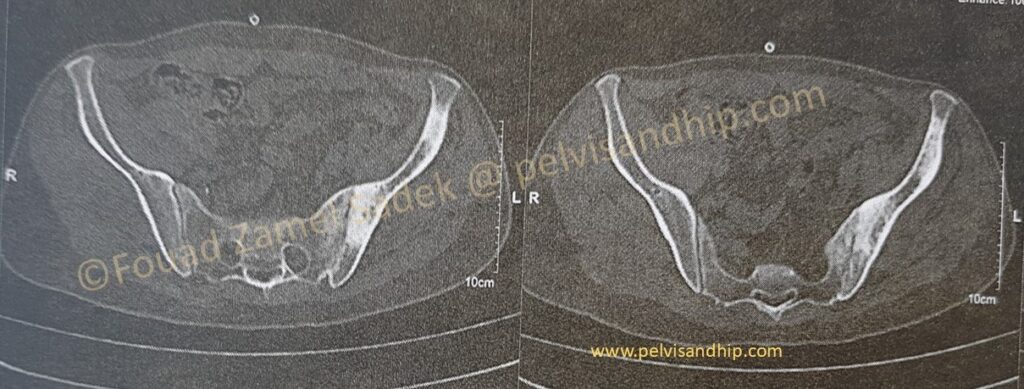
Axial CT cuts reveal a more extensive involvement of the hemipelvis with obvious skeletal changes in response to previous infection including a bony ankylosis of the left SI joint with some extension of the bone reaction in the ilium.
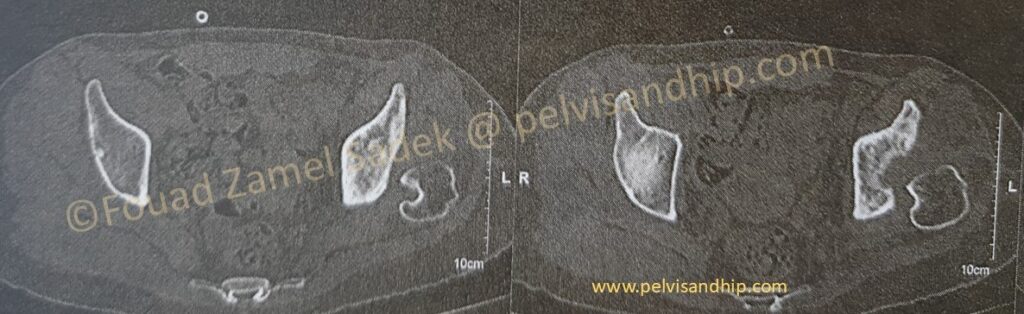
The dome level cuts of the acetabulum again confirms residual bone changes from the previous infection. This is also the best cuts to assess superior bone support and we can easily identify the superior defect at the level of the dome something that could very well require some form of reconstruction.
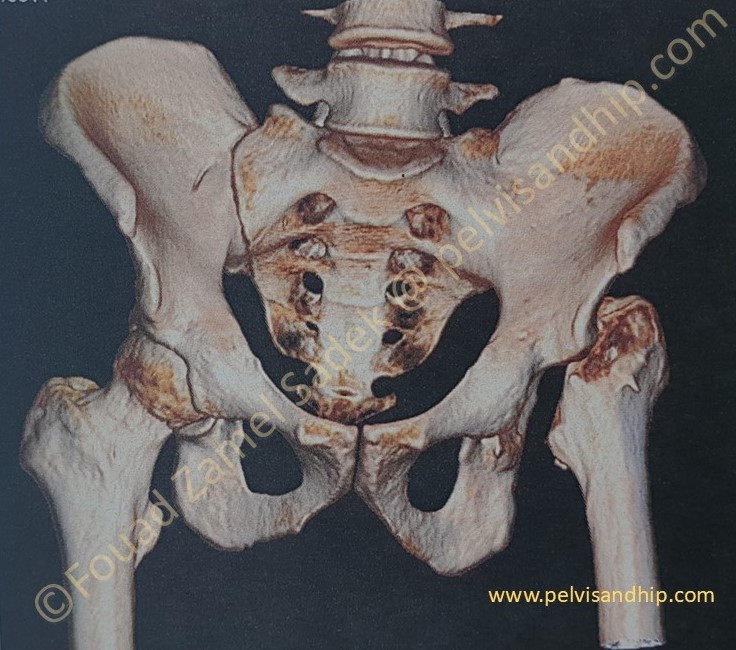
The 3D reconstruction is a very valuable tool for acetabular reconstruction planning. The left SI joint is obviously ankylosed. The anterior wall of the left acetabulum is quite sufficient with no deficiency. The projection of the posterior wall (which is visible in this view due to the absence of the femoral head) can be seen to have some slight deficiency. The upward migration of the left femur is also obvious and may represent some surgical challenges to bring the down the centre of rotation of the reconstructed hip.
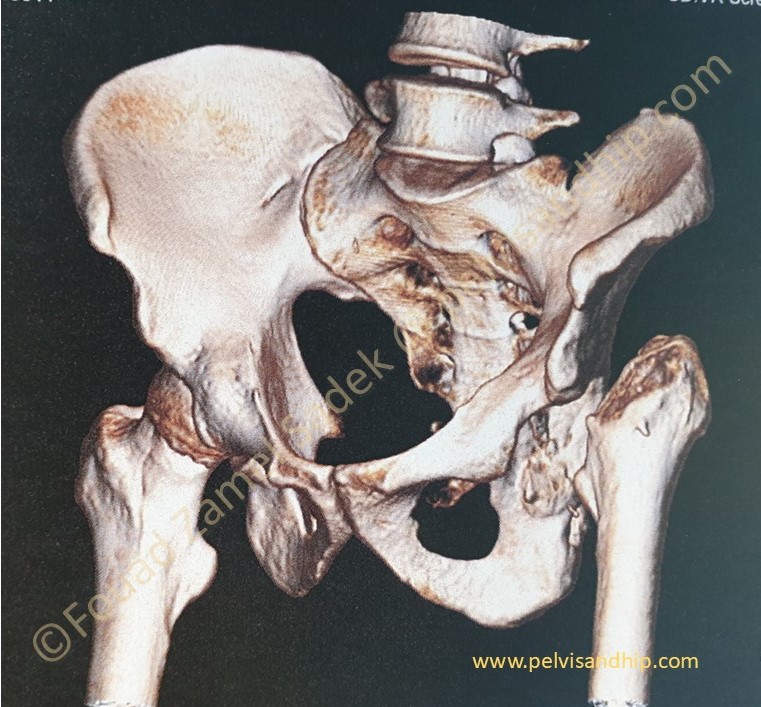
The oblique view of the this 3D reconstruction again confirms the left SI joint ankylosis. It also brings in profile the superior dome which shows its deficiency.
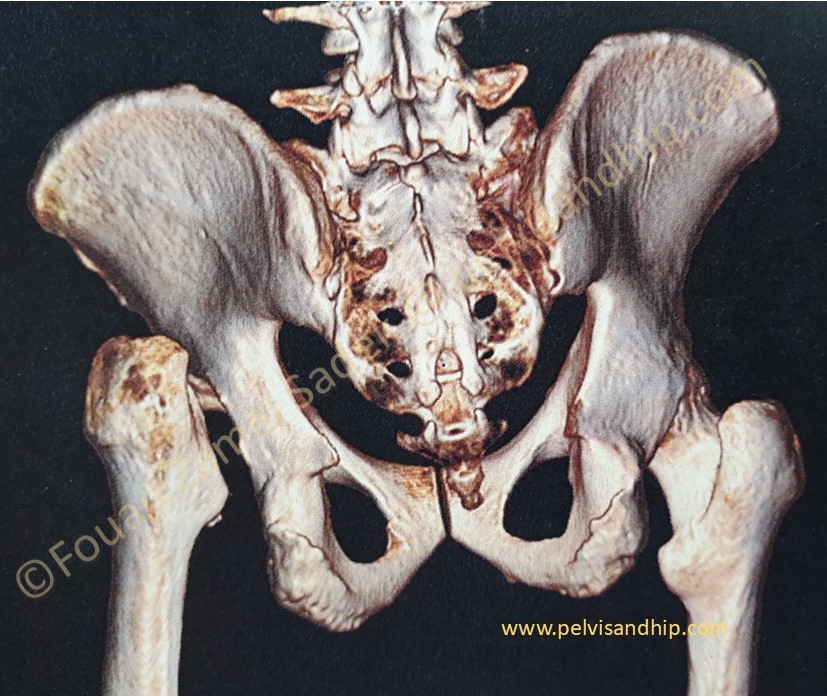
The posterior view of the 3D reconstruction confirms again the posterior wall deficiency by comparison to the contralateral right hip posterior wall.

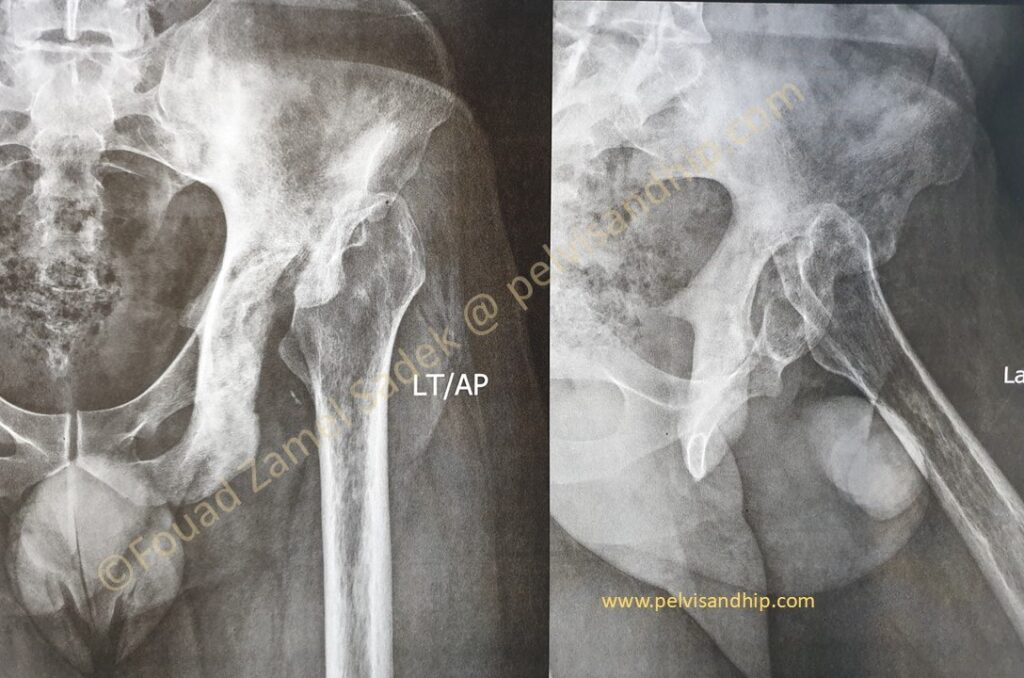
The obvious leg length discrepancy on the left side. The scar of previous interventions suggest some lateral based surgical approach which is well healed with no obvious suspicion of active inflammation.
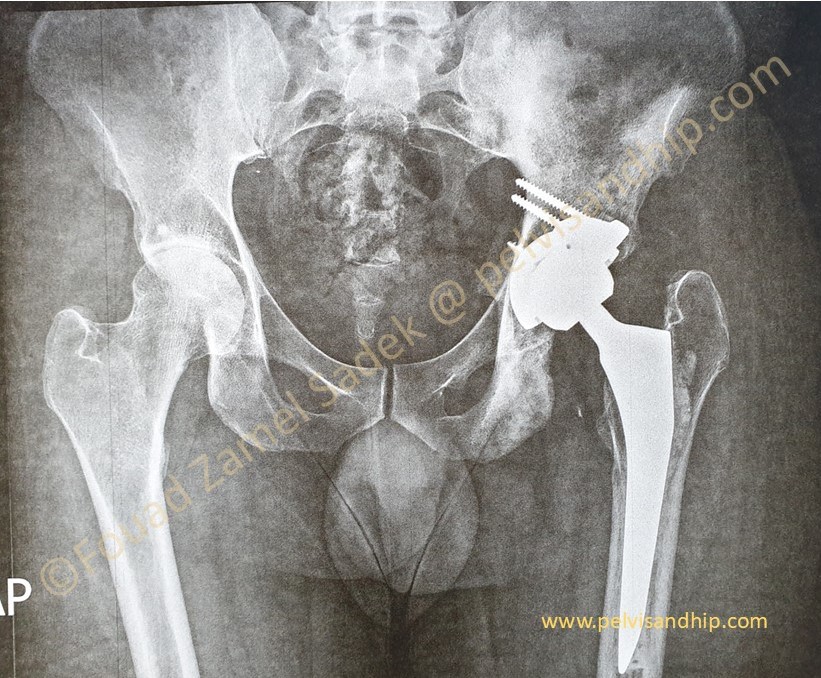
Through a posterior approach, the true acetabulum was identified and cleared of all haling tissues and debris. Radical releases including the postero superior as well as the inferior capsules were done. A periacetabular release procedure was carried out with additional releases of the gluteal maximus attachment into the gluteal tuberosity of the femur. A superior trabecular metal augment was applied as per routine. A porous coated cementless spherical cup was inserted close to the TAL. No further grafting was needed.
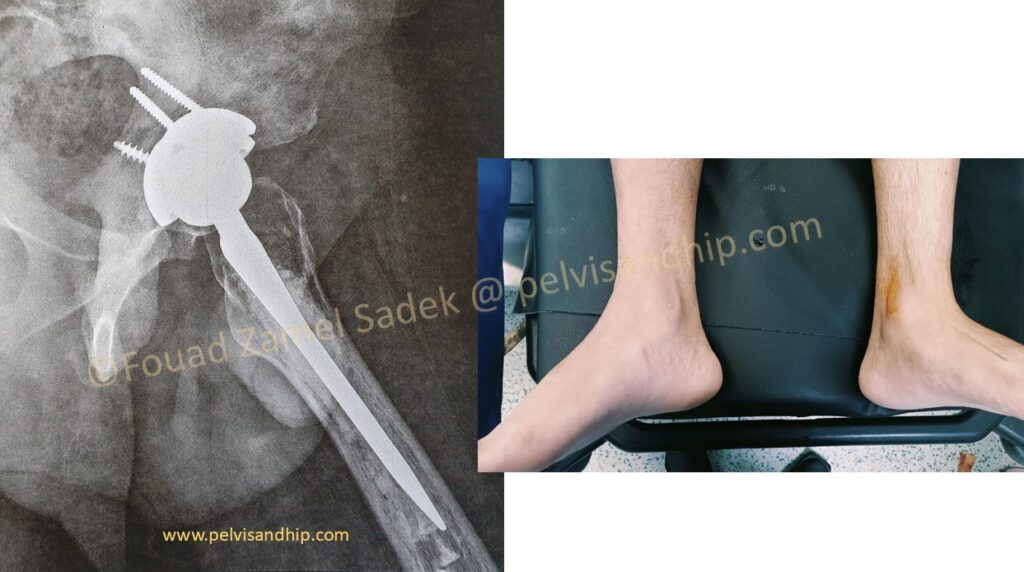
A cemented stem was chosen due to very poor quality bone withing the metaphysis of the femur and for that a cemented option for the femoral stem was chosen. The leg length adjusted as per immediate postoperative finding. At the last follow up, patient is walking with no support. He has a very reasonable abduction function. He has returned to work with good satisfaction. Still working on improving his abduction function.