

This 28 years old young male had previous attempt of curettage somewhere else from this lesion. Further studies confirmed a recurrent chondrosarcoma of the right anterior column of the acetabulum. The plan with our musculoskeletal oncology expert team was to proceed with resection with safety margin and reconstruction of the acetabulum.

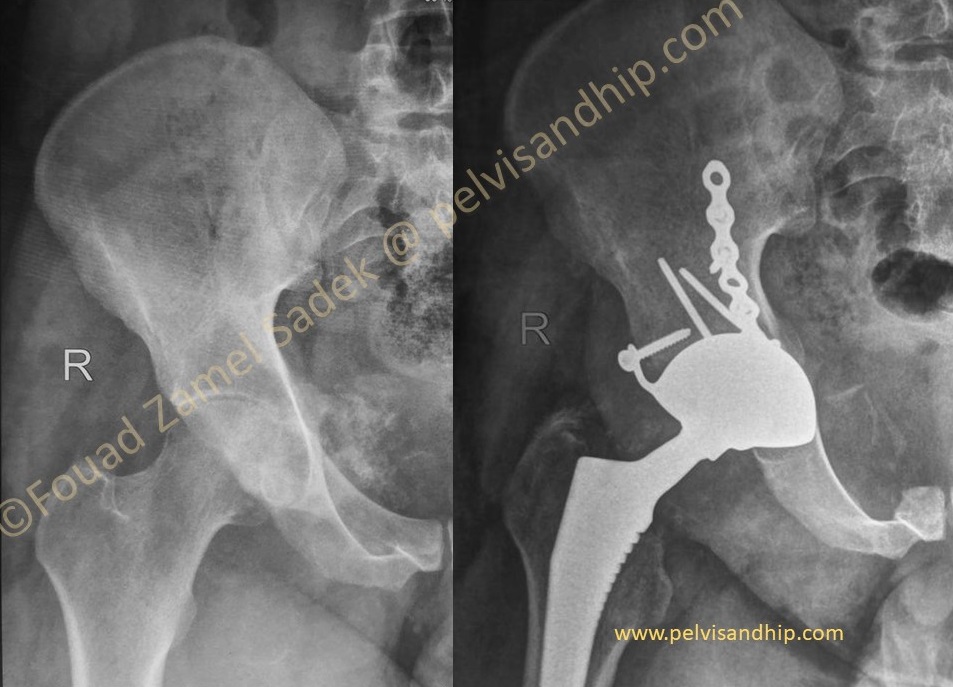
The MRI scan confirms the exfoliative nature of this lesion arising from the anterior column of the acetabulum with what suggests like a clear margin for resection. Such a procedure would entail resection of a significant part of the anterior column of the right acetabulum with a plan for a total hip implantation with acetabular reconstruction. As per previous cases that resection would leave for us the femoral head to be used an autograft for the defect with possible implantation of a standard implant.

A longitudinal incision was used for identification and preservation of the neurovascular tree followed by a wide marginal resection of the lesion including the anterior column of the acetabulum. Through the same rather medial longitudinal incision a cementless dual mobility cup was inserted on top of a femoral autograft which was fixed on the inner side of the ilium with a reconstruction plate (blue arrow). A cementless stem was inserted through a deep dissection similar to a direct anterior approach. The cementless dual mobility cup was chosen for stability considering the soft tissue resection that was part of the lesion excision.

Postoperatively there was an apparent starting sloughing of the anterior wound considering a previous incision with the first attempt of excision. A few days down the line a rotational flap was fashioned and executed to ensure protection of the reconstruction and minimize any infection risks.
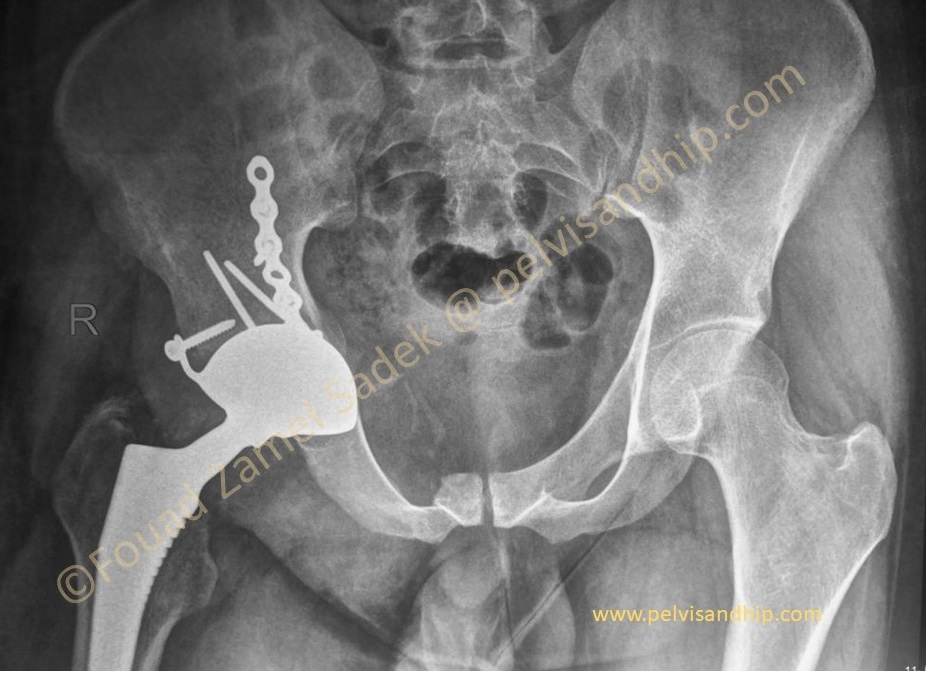
Follow up x-rays with good healing of the surgical approach and good incorporation of the implant with osteointegration of the cup and union of the graft (blue arrow)

Another follow up x-rays after one year and one can appreciate an intact abductor power with no lurch or limping for this young man. The benefit of this abductor preserving procedure can be well appreciated in the face of the clinical result of this patient.
The learning points of this case: 1.Good preoperative planning is very essential to consider not only the resection procedure but also the options of reconstruction. 2.In this case a longitudinal incision was equally versatile and allowed both resection and implantation. 3.Bulk femoral head autograft can be useful in such reconstruction as it tends to behave differently from bulk allograft. 4.A cementless dual mobility cup can be quite useful to provide stability considering the soft tissue resection. 5.Experience with the Direct anterior approach can be tailored and used for implantation of such cases with preservation of the posterior capsule and soft tissue envelope for better stability and better function. Noted by the good abductor function of the patient. 6.Team work is the key to success in any complex case.