

Young doctor subjected to a road traffic accident after which she suffered from this associated pelvis and acetabular fracture. This a vertical shear fracture with dislocation of the right SI joint with upward migration. The contralateral pubic rami are fractured. The right acetabulum is fractured with what looks like a transverse fracture. The status of the posterior wall is not very clear in this view. The young lady had right sided foot drop with what looks like a lumbo sacral trunk injury

A close view of the right SI joint confirms the overlap of the ilium to the sacral ala. Upward dislocation of the SI jotni is obvious.
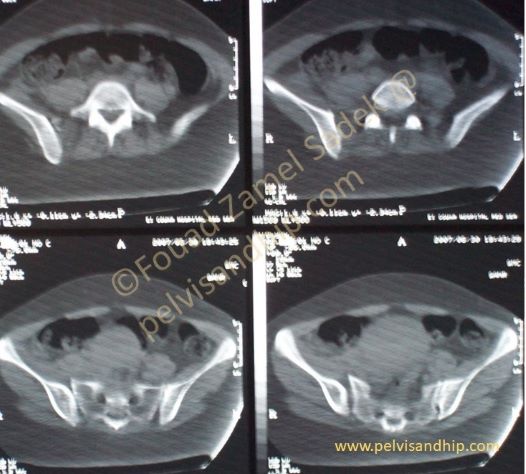
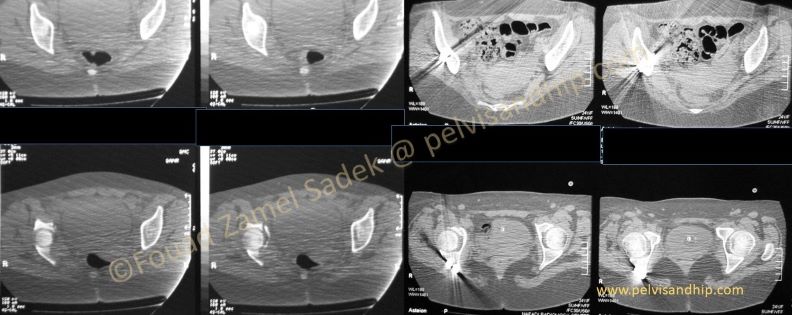
Following the axial CT scan reveals the incongruence of the right SI joint and the gapping of the joint.
Clear widening of the dislocated right SI joint is quite obvious in these CT cuts.

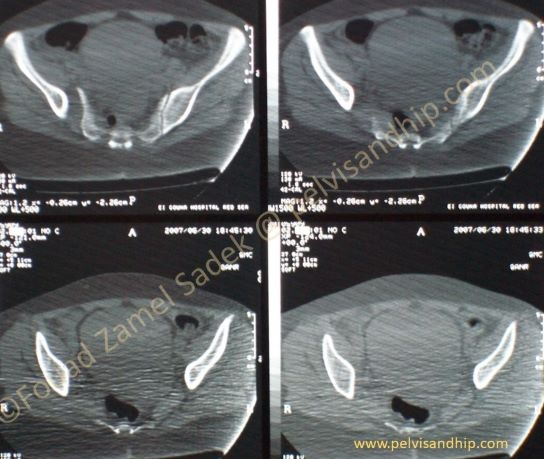
The axial CT cuts through the right acetabulum confirms the transverse nature of the acetabulum with what looks like a posterior wall fracture that needs to be tended to.

The initial treating surgeon considered the right sided foot drop like an emergency with what looked like an anterior approach to the right SI joint an attempt was made at open reduction and internal fixation of the SI dislocation with no concern for either the anterior ring or the associated transverse with posterior wall fracture of the right acetabulum. Further more one can clearly recognize the malreduction of the SI joint with residual displacement both upwards and posteriorly.
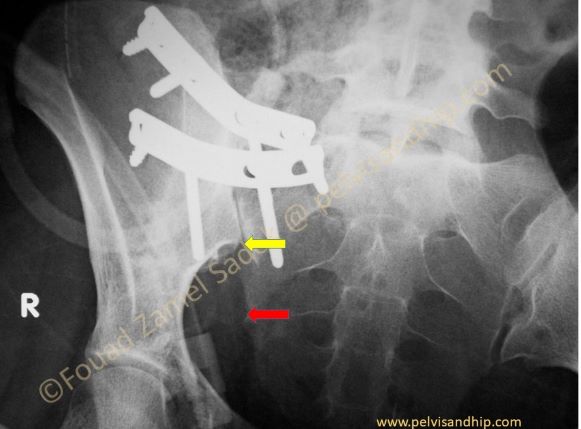
The outlet view with a close up view confirms the malreduction. Notice the significant gap between the reduced position of the ilium (yellow arrow) and the anatomical position it needs to be reduced to (red arrow). Such a reduction can obviously not be tolerated.
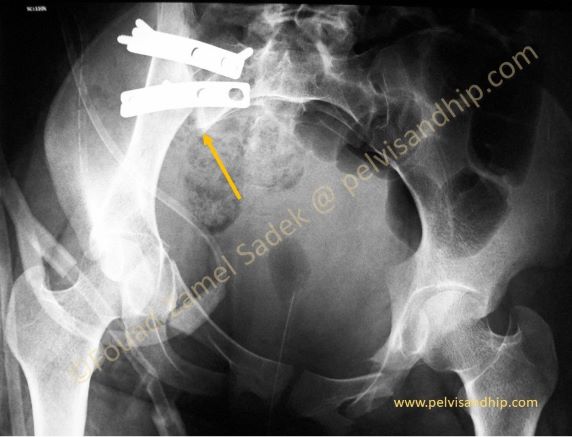
The inlet view of the pelvis also shows the distorted pelvic ring with malreduction. The ilium is still posteriorly displaced which is needs to be revised and reduced in place.

Patient was approached after 3 weeks from the first surgery first in the supine position with anterior approach to the right SI joint. The two previous plates were removed and the SI joint was anatomically reduced. Fixation was done with an SI screw in addition to two anterior plates to the SI joints.
Patient was turned in the prone position to approach the acetabular fracture which was reduced and internally fixed as per routine. Then an anterior inferior iliac spine external fixator was applied to complete the pelvic stabilization of the anterior ring.

The inlet view confirms the adequate reduction of the SI joint (arrow)

These two close up pictures are put side by side to appreciate the difference in reduction between the first surgery on the left and the second corrective surgery the right. This outlet view shows clearly the well reduced SI joint on the right. Notice the position of the two sacral screws of the plates (arrows) showing the ideal positioning of these two screws whenever we plate the SI joint anteriorly.

Notice the corrected position of the SI joint on the inlet view on the left side with adequate reduction and fixation of the SI joint.

This AP view of the pelvis shows clearly the overall final picture after removal of the external fixator with satisfactory and reduction and fixation of both the pelvis and acetabular injuries. Notice the anatomical reduction of the transverse acetabular fracture as well. The contralateral pubic ramus fracture is also united.
This postoperative CT scan on the right picture shows clearly the anatomical reduction of the acetabular fracture with the adequate placement of the posterior plate.

Learning points: 1. associated pelvis and acetabular injuries are complex injuries that need to be approach in total.
2. The pelvis injury has to be reduced and fixed first before embarking on any associated acetabular fractures. 3. Anatomical reduction of an SI joint can be tricky and one should not fix malreduced joints. 4. Anterior ring injuries are an important component of the pelvis ring as a whole and therefore call for complete fixation of all components of the ring injury; in this case an anterior external fixator was used.

If you feel like posting comments, enquiries or questions please click here.