

37 years old male having a cementless total hip replacement done for femoral head damage following a complication of previous surgery for a femoral neck fracture. Patient had a corail cementless stem with a pinnacle cup inserted. Patient a delta ceramic on ceramic 36mm head. Surgery was done in a routine way with no apparent complications.
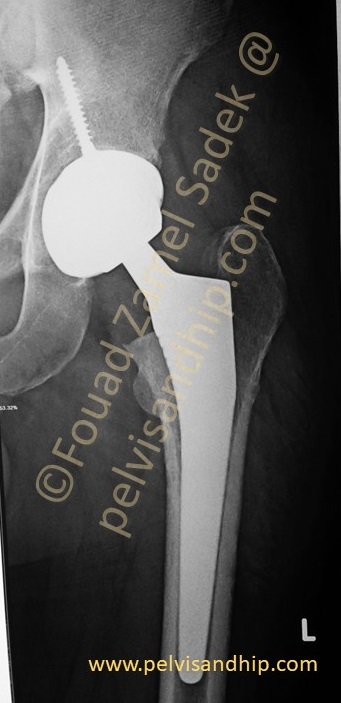
Patient was reviewed at 2 months with the follow up x-rays which was satisfactory with no complaint and patient has been walking full weight bearing.

One month later patient presented with a sudden gradual sinking of the stem. There was no obvious history of any trauma except a first time attack of epilepsy. Patient had not been diagnosed before with epileptic fits and family history reported a long first attack extending to around almost 15 minutes. Personal explanation was that the clonic uncontrolled muscular contraction of a ceramic on ceramic head might have provoked destabilization of the stem. Patient was not complaining of any pain in the hip but only shortening on the side of surgery. He was advised to come back for revision which he didn’t do and presented for revision surgery after another 5 months

At 8 months after the index surgery, introperative attempt of femoral stem removal as an endofemoral procedure with multiple drilling and using k-wires failed. For which a short extended trochanteric osteotomy was done to by pass the bend part of the stem to allow and easier drilling around the stem. This was done with a desire to have a short stem revision rather than a formal ETO that would need a long stem revision in a such a young active patient. The osteotomy revealed a very extensive layer of bone formation around the femoral stem HA coating which encouraged us to preserve such a perfectly oteointegrated stem in a such a young active patient.

The plan changed into preservation of the femoral stem with advancement of the greater trochanter and its reattachment. This was followed by application of a long femoral neck to compensate for the sinking of the femoral stem. This corrected for his shortening and preserved the same stable stem he has been using. On follow up x-rays showed complete union of the trochanteric osteotomy. He was satisfied and this procedure offered the same stem with its longevity potential.

Learning points: 1.Careful study of any failed total hip requires assessment of symptoms. In this case there is shortening with no pain. 2.HA coated well reputed stems can have extensive osseointegration with very good stable constructs that should be considered in any revision procedure 3.An extended trochanteric osteotomy is a very versatile procedure that can be used and tailored in different ways according to the different clinical scenarios 4.Innovative solutions can provide the patients with the needed results depending on the clinical condition; in this case avoiding a long stem revision and preserving a well integrated primary stem.

If you feel like posting comments, enquiries or questions please click here.