

This 18 years old young lady suffered from a fall from a height whereby she had this complex injury. A vertical shear fracture pelvis on the left side and what looks on the AP view like a transverse fracture of the left acetabulum as well. Both injuries are 4 weeks old and were neglected without any intervention. The left femoral neck fracture was fixed with these 2 cannulated screws which although may look like adequately fixed other views show otherwise. The left SI joint is dislocated with upward migration. There is a disruption of the symphysis with contralateral fractures of both rami.

The inlet view shows clearly the dislocated left SI joint with posterior displacement of the left hemipelvis in relation to the sacrum. The displacement of the acetabulum is clear with lack of congruence of the left acetabulum. The left hemipelvis is also internally rotated.

Outlet view of the pelvis shows the vertical displacement of the pelvis and on this view the hemipelvis is sort of adducted. The view is not perfect as an outlet view. The transverse process of the 5th lumbar vertebral is fractured. On this view one can start to appreciate the dysmorphic sacrum.

This iliac oblique view shows the fracture involving the posterior column which is the posterior extension of the transverse fracture of the left acetabulum.

The obturator oblique view confirms the transverse fracture of the acetabulum showing the anterior column component. On this view one may start to consider the odd position of the superior screw of the femoral neck.
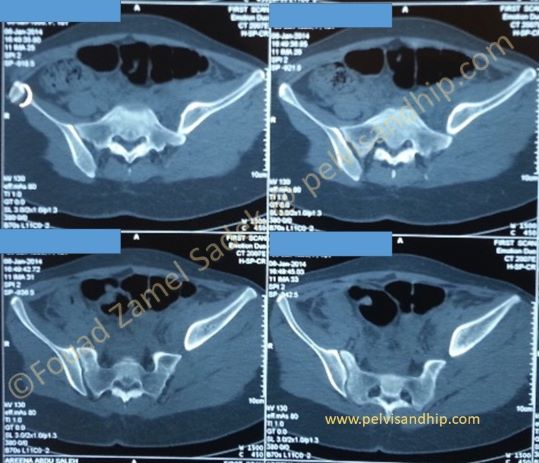
The axial CT scan shows the dislocation of the left hemipelvis in a very proximally migrated position. The first sacral segment is clearly dysmorphic whereby a transversely placed SI screws cannot be inserted safely to cross the midline.

CT scan of the pelvis showing both the anterior position of the ilium as well as the acetabular fracture. On the lower right quadrant a possible intraarticular screw end can be seen posterior to the femoral head (red arrow)

3D reconstruction showing on the front view the vertical fracture of the pelvis. The SI joint dislocation is very significant with upward and posterior dislocation. (red arrow) The transverse fracture of the acetabulum (yellow arrow) is clear with medial displacement. The position of the proximal ilium is the probable reason for the lack of congruence of the hip joint.

3D reconstruction viewed from the back showing the posterior column fracture of the transverse fracture. On this view you can see the position of the posterior femoral neck screw which is outside the neck and in the joint. (arrow)
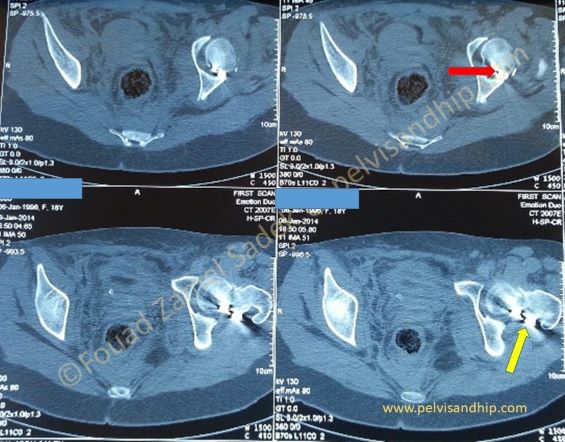
On the axial CT view, there is an obvious screw (red arrow) in the joint posteriorly. Also, the screw at the level of the neck is outside the posterior cortex (yellow arrow)

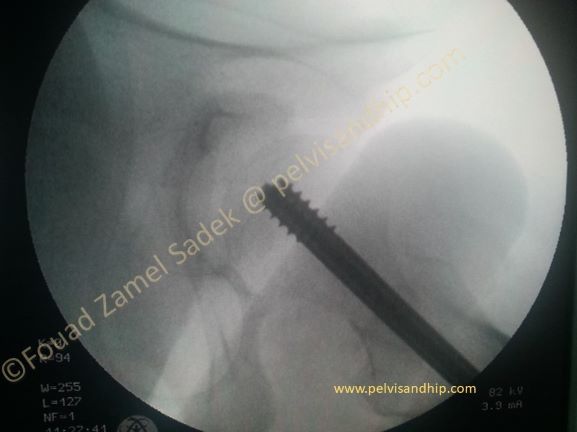
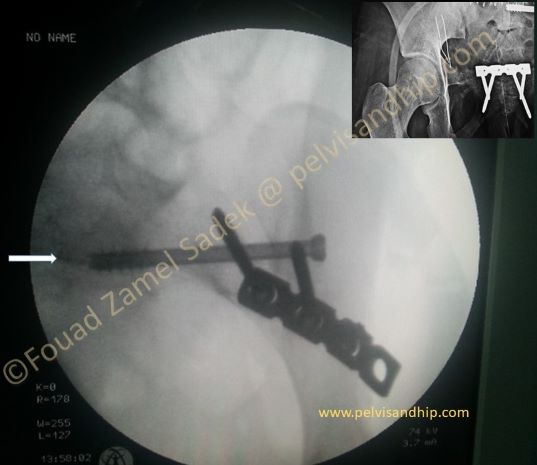
Lateral view on fluoroscopy shows the posterior screw of the femoral neck outside the neck and reaching the joint. (arrow)

The femoral neck is well reduced but the screw fixation is not adequate. The posterior screw is removed first.

Before changing the position of the second screw another guide is inserted in the ideal position to fixe the neck and guide the other screws to be inserted.

2 new different screws were inserted without changing the reduction of the femoral neck which was satisfactory.
In the lateral view the screw positions are satisfactory. The reduction is acceptable. The femoral narrow is too narrow to take a third screw.
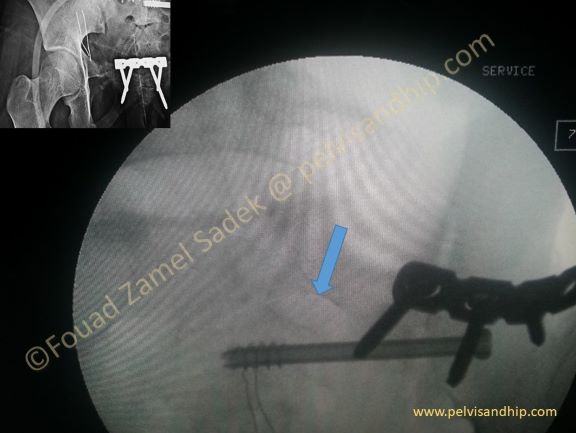
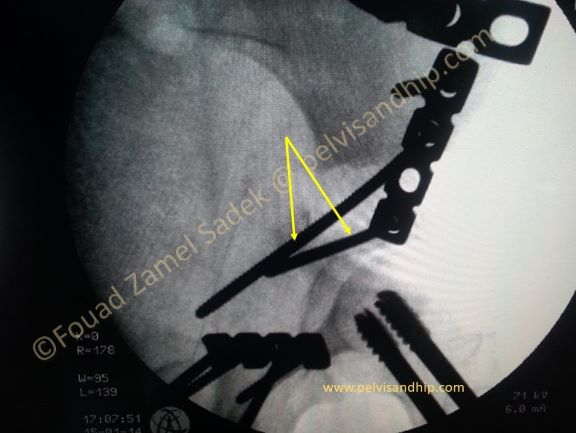
Through an ilioinguinal approach the left SI joint was exposed and reduction was done to a satisfactory position. This was done after reduction and fixation of the symphysis with plates and screws (inset picture). In addiction to the SI plate a sacroiliac screw was inserted in the S2 position as the sacrum was seen to be dysmporphic. The fist sacral foramen can be clearly seen (arrow)
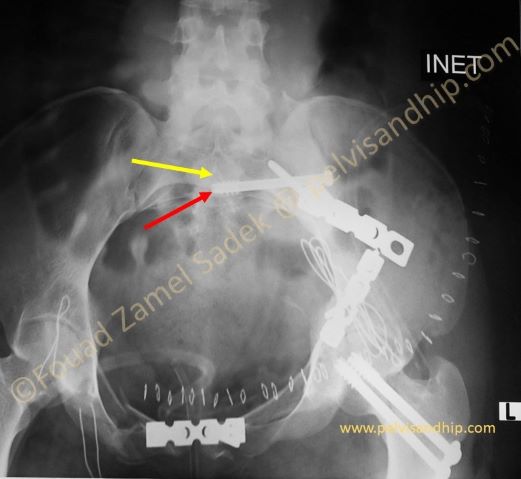
The SI screw in the inlet view is in the right position. The shadow of the body which is transgressed with the tip of the screw is not the body where the screw resides. This ridge is that of the upper vertebral body namely S1 body (arrow). The screw was inserted into S2 as this is the more capacious body; S1 is dysmorphic and although sometimes one can insert a screw into this body it is not ideal for long screws that reach the midline.

Closure of the transverse fracture was done with the large pelvic reduction clamp with one tong outside the ilium and the other longer one through the middle window of the iliinguinal approach was applied on the transverse fracture to close it. An attempt was thought of to fix the anterior column with an anterior column screw but the very narrow pubic ramus made us change the plan.

Obturator view of the hip shows the adequate reduction and fixation of the anterior column. These screws were changed with screws into the posterior column.
An iliac oblique views shows the ideal positions of the distal 2 screws of the plate fixing the posterior column from the front position. (arrows)

The final reconstruction shows the anatomical reduction of all fractures; the pelvis fracture is fixed with one anterior SI plate with an S2 screw and a symphyseal plate. Note that with 3.5mm reconstruction plates the ideal positions for the screws criss-crossing the pubic bones. The femoral neck is well reduced and fixed. The transverse acetabular fracture is reduced and fixed with short segment fixation (a plate short of the iliopectineal eminence). Well placed ilioischial screws look on the AP view of the pelvis to be along the long axis of the ischium (long arrow)
The inlet view showing the adequate reduction and fixation of the pelvis. The SI screw is inserted in the second body (red arrow); S1 body is smaller and showing the characteristic recession of the fist sacral body (yellow arrow)

Learning points:
1. Complex injuries have to be completely and globally managed.
2. Associated pelvis and acetabular fractures require special handling and understanding; such injuries are more than the summation of each injury.
3. We recommend reduction and fixation of pelvic injuries first before working on the acetabular fractures.
4. Beware of sacral dysmorphism when using sacro-iliac screws.
5. Short segment fixation has become one of our popular technique for fixation of most anterior column fractures; this means a short plate which doesn’t go beyond the ilipectineal eminence.
6. Careful technique allows posterior column fixation from the front with well placed targeted ilio-ischial screws.

If you feel like posting comments, enquiries or questions please click here.