
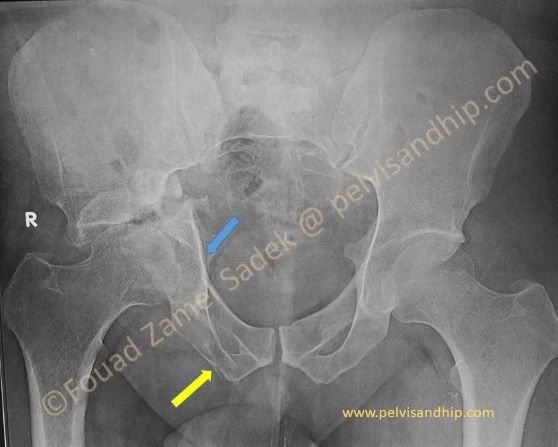
AP view of the pelvis in a 37 years old male 7 months after an RTA. Patient had no initial treatment. On this view, there an associated T fracture with a posterior wall although one can think of it as a transverse fracture. The crossing of the iliopectineal and ilioischial lines (blue arrow) in addition to the fracture of the pubic ramus (yellow arrow) suggests a T. The posterior wall can be seen above the femoral head which is centrally dislocated.

Iliac oblique view showing the probable cartilage damage of the joint with the displacement of the posterior column. The apparently spherical femoral head made the patient ask for a trial of hip preservation.
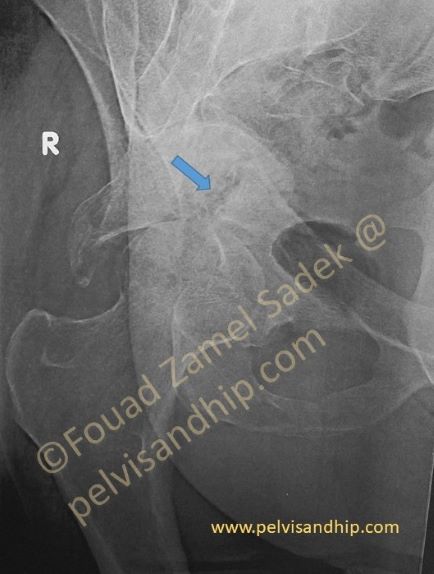
The iliac oblique view shows the anterior column displacement as well the associated posterior wall. On this view a persistent non-union (arrow) is suggested. The femoral head has been abutting on the fracture plane in this dislocated position.
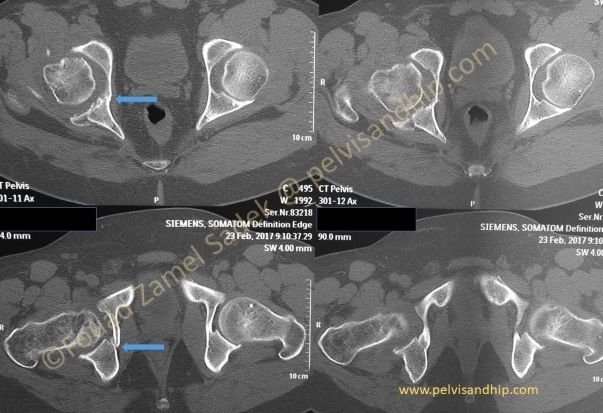
Axial CT scans show that the femoral head may be more damaged than it looks on the x-rays studies. You can see the vertical fracture plane that makes this fracture a T fracture rather than a transverse one. (arrows)
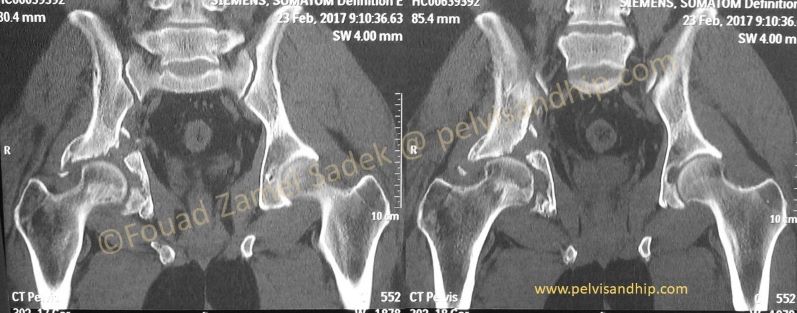
The coronal reconstruction confirms the non-union of the transverse component of the fracture which makes it more feasible to reduce and fix the fracture from a single approach in this case a posterior approach with an easier mobilization of the fracture going intraarticular and curetting the fracture plane.
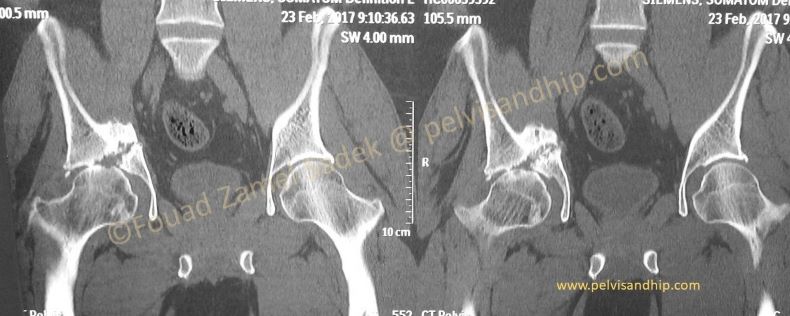
On this other coronal cut the fracture doesn’t show a uniting bony bridge confirming non-union. The femoral head on this view suggests more damage than anticipated.

The posterior view of the 3D reconstruction shows the posterior column of the fracture as well as the posterior wall. There a superior segmental defect in addition that would probably need a femoral head autograft. The surgical plan is to mobilize the fracture to complete the acetabular sphericity, use the femoral head to graft the posterior wall segmental defect and insert a cementless press fit cup after fracture fixation.
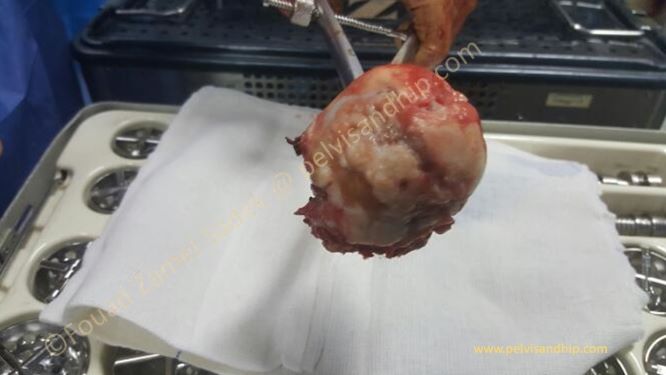
Intraoperatively the damage of the femoral head could be easily identified with early femoral neck resection prior to acetabular exposure, mobilization and preparation.

A press fit cementless cup was inserted after reduction and fixation of the transverse component with a 3.5 reconstruction plate. The aim was to complete the sphericity of the acetabulum for the cup implantation. A stable press fit insertion is mandatory and screws are only used as an optional choice for further stabilization.

The lateral view of the hip shows satisfactory seating of the cup with good posterior column contact directly to the acetabular component. Extra screws in the cup can also be used to increase stability not only of the cup but of the fracture as well.

Points of learning: 1.The final judgement of viability and adequacy of a dislocated femoral head, can only be done with certainty intraoperatively. 2.Careful study for neglected cases can be improved with CT scans to assess union which may influence surgical plan including approach 3.A reasonable technique for acetabular reconstruction in selected cases is to perform delayed open reduction and internal fixation of the acetabular fracture. Mobilization of the fracture allows the completion of the acetabular sphericity for press fit cup implantation.

If you feel like posting comments, enquiries or questions please click here.