

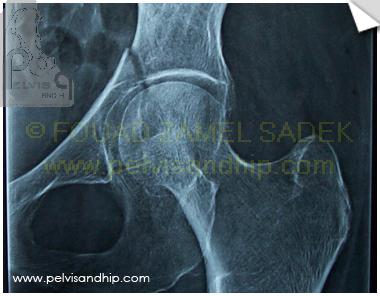
An antero-posterior view of the pelvis showing an associated transverse with posterior wall acetabular fracture. An active 72 years old lady going up hill at the pyramids, hit by a taxi. she has never complained of any hip related symptoms prior to the injury. No other associated injuries. A single projection of this view shows a simpler injury pattern than what it really is.
On the obturator oblique view the maximum displacement of the anterior column component of the transverse fracture which is juxtatectal can be revealed. The posterior wall seen at its best in profile on this view is not signficantly displaced; but another fracture characteristic will be revealed on CT scan.
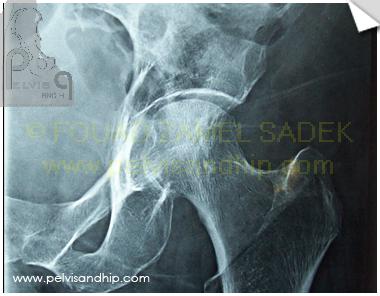
An inadequate iliac oblique view shows the posterior column not in its best projection with no major displacement.

The axial CT cut shows the top extension of the anterior column part to go just beyong the dome of the acetabulum (a ? transtectal fracture)

Going lower down through the joint, though the undisplaced nature of the posterior wall is confirmed, another pattern of the injury is revealed with the most upper extension of a marginally impacted fragment under cover of the undisplaced fracture of the wall.

Further down the marginally impacted fragment reveals its rather large size and its position in a critically important part of the posterior articular acetabulum

More distally, the marginal impaction fragment is clearly delineated at the level of the ischial spine between the posterior wall and the lesser sciatic notch part of the posterior column

Further down, marginal impaction extends into the column just above the ischial tuberosity; denoting how significantly large the fragment is.

A good size articular component is seen on this view with a clearer delineation of the fragment. The lower limit of the posterior wall fragment is almost reached.

The upper part of the ischial tuberosity is starting, reaching the inferior limit of both the posterior wall and marginal impaction.

The inferior limit of the acetabulum is almost reached just above the obturator foramen and shows how extended the lesions are.

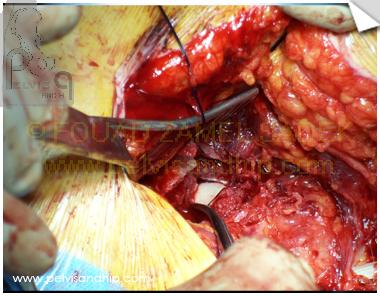
An intraoperative picture of a Kocker-Langenbeck approach, in the prone position,where the top picture is posterior, the right is distal, the bottom part is the anterior edge where the surgeon’s hand is seen and the left side is the proximal part. Notice the tip of a curved artery inserted in the gap resulting from the displaced margnial impaction just posterior to the femoral head (white cartilage in the middle).

After elevation of the marginally impacted fragment and its reposition on the femoral head (small cartilage part is seen); the curved artery is now inserted behind the fragment in its cancellous bed with introduction of some bone graft chips taken from the greater trochanter.
The fragment is now well repositioned on the femoral head and well supported in its place by the bone graft filling the void which was behind it. Notice that in order to get access to this fragment, the minimally displaced posterior wall fragment had to be fully elevated and displaced carefully from its bed and then reduced anatomically back.
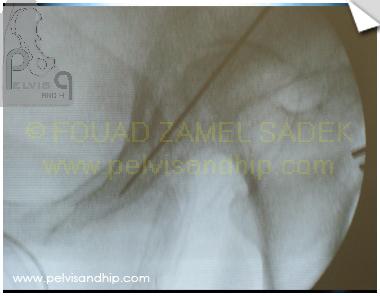
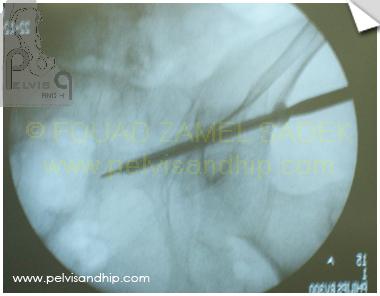
To improve fixation and attempt at reducing the anterior column part by lag effect; an anterior column screw was attempted prior to plate application; to have more freedom in the choice of entry point since the ideal place of a posterior plate may occasionally interfere with the ideal entry point of the column screw. On this iliac inlet view the guide wire can be seen in a good position.

The cannulated drill bit is seen carefully introduced over the guide wire on this obturator outlet view just above the joint and below the vessels.
Closure the gap and fixation of the fracture is completed as per routine with tightening of cannulated partially threaded 7mm screw with the use of a washer.
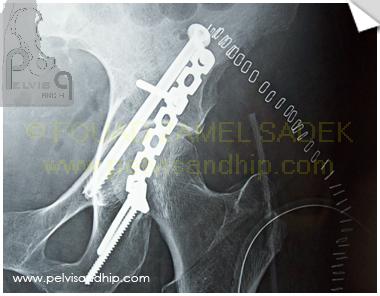
The final postoperative picture as seen after fixation with the posterior plate and the anterior column screw in place.

The obturator outlet view shows the adequate placement of the screw. A 7mm screw is close to the size of an anterior column in such a lady but with careful intraoperative imaging a centralized position of the screw can be safely obtained. The 3.5mm reconstruction plate is carefully contoured over the posterior wall.

An antero-posterior view of the pelvis with some tilting towards an outlet view showing the reduction and hardware placement. On the greater trochanter one can see the window of the graft just at about the level of the vastus lateralis ridge.

A semi-inlet view of the pelvis showing the reduction and fixation of the fracture. Patient is allowed bed to chair with touch weight bearing mobilization.

If you feel like posting comments, enquiries or questions please click here.