

AP view of an associated acetabular and pelvic fracture in a 14 years old young girl. Pelvic fracture is a vertical shear. Posterior ring failure is a fracture disolcation not amenable for SI screw fixation. In addition to the contralateral superior pubic ramus fracture there is an ipsilateral fracture of the left acetabulum; a transverse fracture with anterior column displacement more than the posterior which is in place.

On the inlet view, the fracture dispacement of the pelvis is obvious. The acetabular fracture is displaced which is not ideal to ignore in such a young lady of 14.

The oulet view (not ideal), shows the displaced fracture dislocation of the left SI joint more clearly. The displaced acetabular fracture is evident. Surgical reduction and fixation are indicated. The plan is for an anterior SI joint approach for both reduction and fixation. The acetabular fracture can be fixed by extending the incision into an ilioinguinal approach in classic teaching. Another option is available however.
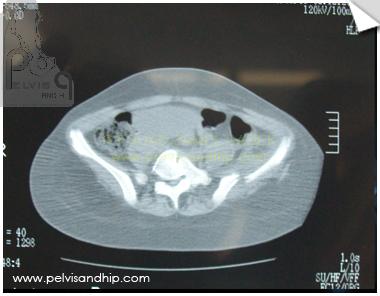
The axial CT cut identifies the nature of the SI joint fracture dislocation with a very high fracture of the ilium seen.
Going lower down the SI joint start to be seen with the fracture of the ilium depicted.

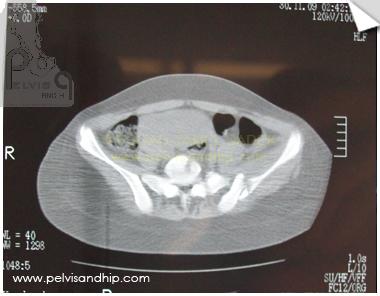
The nature of the fracture dislocation can be well seen as we are going lower down.
The inferior part of the SI joint shows the widening of the joint which confirms that the injury at the inferior level is not a pure ilium fracture.

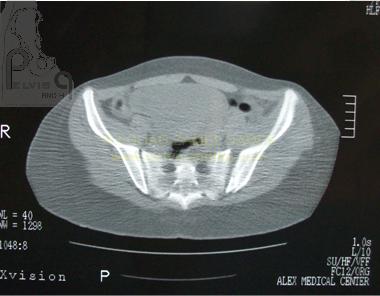
Further down the signficant widening of the SI joint can be identified clearly.

Just above the dome of the left acetabulum the anterior column top part of the displacement can be seen.

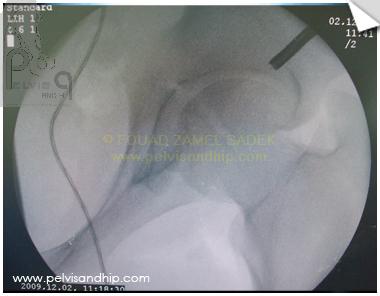
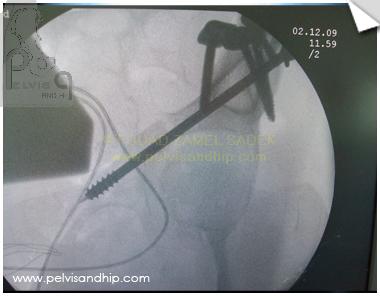
An obturator oblique view done intraoperatively with image intensifier clearly shows the degree of anterior column displacement with an obvious gap in a juxta tectal location. This view was taken prior to any reduction or fixation of the SI joint injury.

Similarly the fracture dislocation of the left SI joint can be seen with the wide gap and displacement.

Through an anterior approach limited to the SI joint only the fracture was reduced and fixed with interfragmentary screws and buttressing plates for stability.

Instead of extending the incision into an ilioinguinal approach. A decision was made for percutaneous fixation as after reduction of the iliac fracture the displacement has been signficantly reduced. Plan is to complete reduction with interfragmentary fixation. Through a separate subcutaneous stab and from the same skin wound, the guide wire is inserted to identify the ideal portal on this oblique obturator view.
Manipulation of the wire can be cumbersome as it bends and may not follow the ideal path. One way of having better control is to start over the guide wire by introducing the drill bit which is much more rigid and can be controlled into the ideal direction as seen on this iliac inlet view.

On the obturator outlet view further confirmation of the position of the drill is seen and the final direction is predicted to be satisfactory.

The cannulated drill bit is then used as a sleeve and the rest of advancement is done first with a long guide wire (we tend to prefer the use of long bayonnet wire similar to the ones used with ring fixators). Advancement of the wire is done carefully under image intensifire until the desired length of introduction is done. On this view it is mandatory to make sure that one is not perforating posterosuperiorly or anteroinferiorly.
The rest of the procedure is done as per routine with drilling over the guide wire followed by introduction of the partially threaded cannulated screw with a washer for completion of reduction and closure of the fracture gap. It is crucial to clearly identify the purely intraosseus path of the screw and confirm the extraarticular nature of this path.

On the iliac inlet view one can identify the position of the screw with satisfactory reduction of the fracture.

3 months postoperatively patient is fully weight bearing with union of the fractures for both the pelvis and acetabulum.
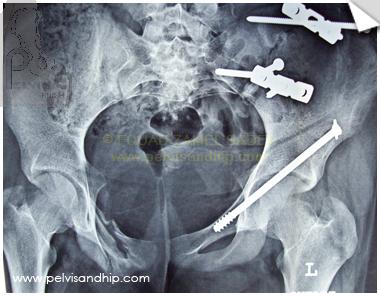
Follow up view of the pelvis. No reduction or fixation was attempted to the contralateral superior pubic ramus which has healed on its own.

Follow up inlet view of the pelvis with good restoration of the pelvic shape and complete union of the fractures. Young lady has a painless full range of motion of the left hip joint.

If you feel like posting comments, enquiries or questions please click here.