
case 13 hip reconstruction

Story starts with a fall 7 years before with a resultant fracture neck of femur which was neglected. Patient states that he was treated with an application of some external fixation for a long time.

It is obvious that he had a Pelvic support osteotomy.
He is currently presenting with difficulty in walking, a significant pelvic tilt and leg length discrepancy. He gets early abductor weakness after any extended walking distance.
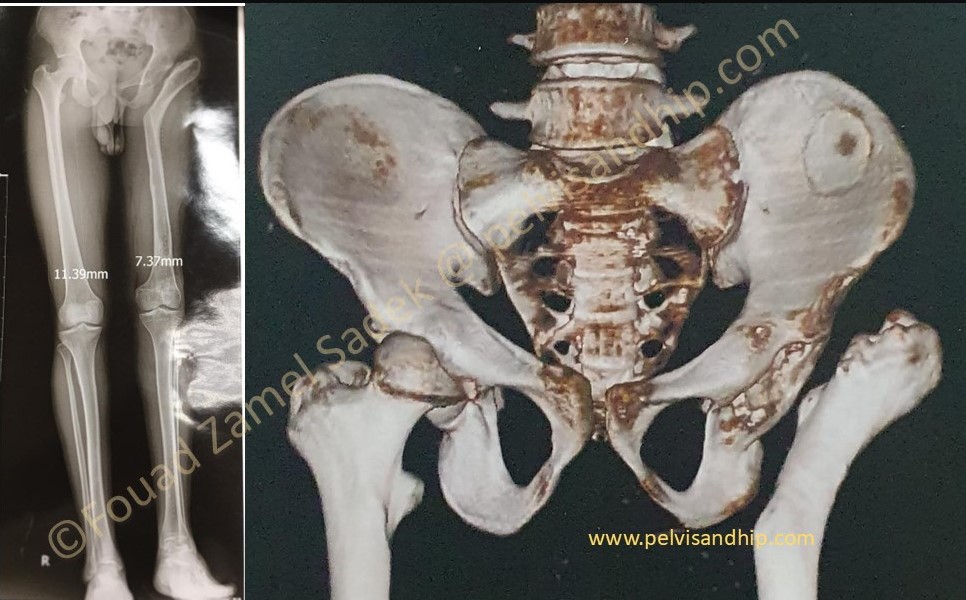
The obvious proximal femoral deformity can be clearly visualized on the 3D CT picture. The standing scanogram also shows the leg length discrepancy and the pelvic tilt. The insufficient adductor lever arm clearly explains the inadequate gait obtained from such a salvage procedure.
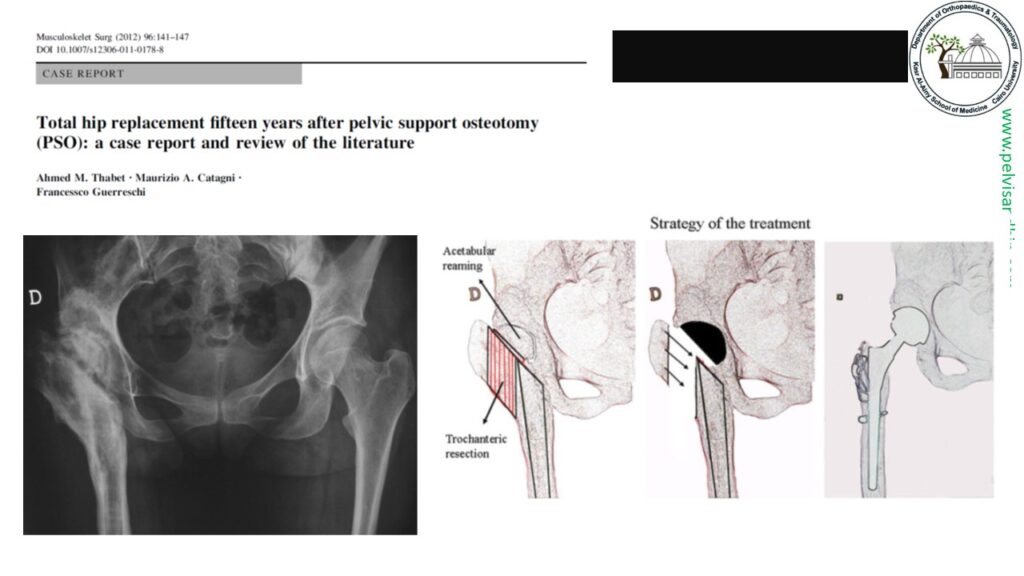
Conversion of pelvic support osteotomies into hip arthroplasty have been very scarcely reported in the literature with occasional single case reports. It has always been recognised that the technical difficulties can be quite challenging.

The technical challenges of the conversion procedure have been well mentioned among which reports of perforations of the femur and extramedullary implantations that required early revision procedures. (The above case is one of such rare case reports)

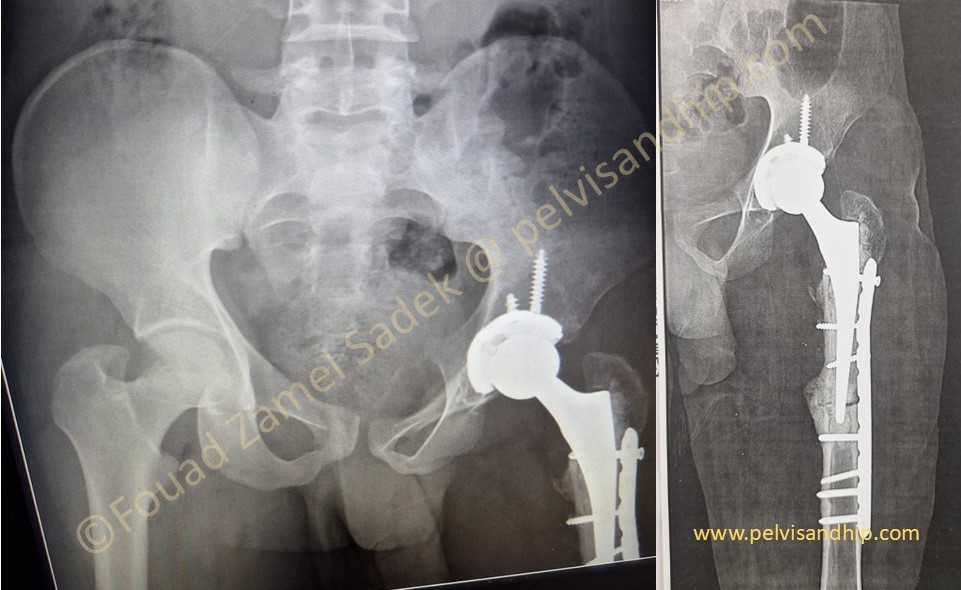
The presented case was operated upon in our pelvic and arthroplasty unit in Cairo University Hospitals. Through a standard posterior approach the cementless acetabular component was safely and well applied. On the femoral side risk of perforation was very high.The choice at hand was between carrying some form of extended trochanteric osteotomy that would preclude the use of a long bypassing stem, which was not ideal for our patient age and level of activity.
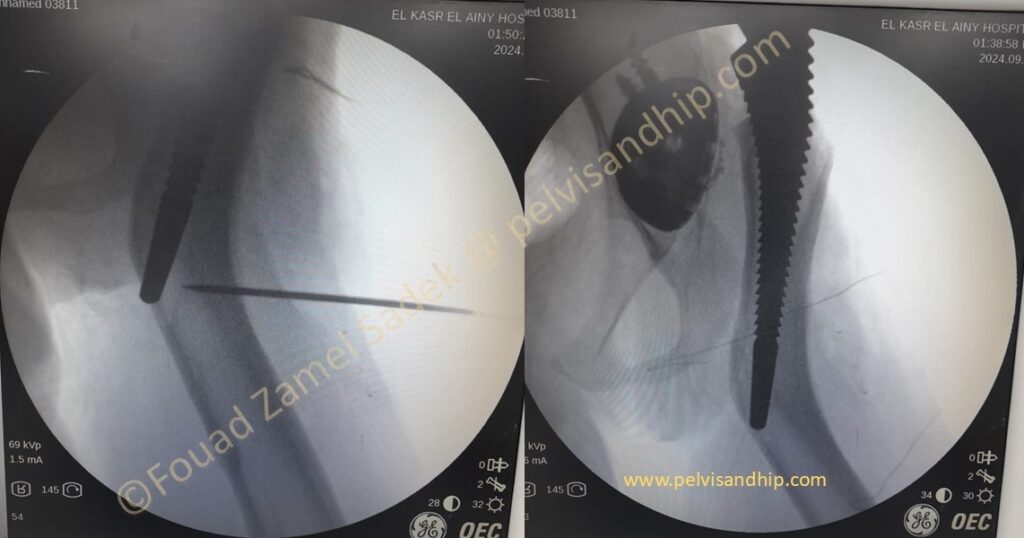
The second was to perform a transverse femoral osteotomy before preparing the medullary canal which increases the surgical difficulty. We opted for another solution. The projection of the endofemoral rasping was identified by drilling along that rasping path with a guide pin followed by drilling with 7mm DHS inner drill of the standard triple reader. That opened a strategically placed cortical window for the distal tip of the femoral rasp. Further gradual rasping could be then carried out with no risk of femoral fracture.
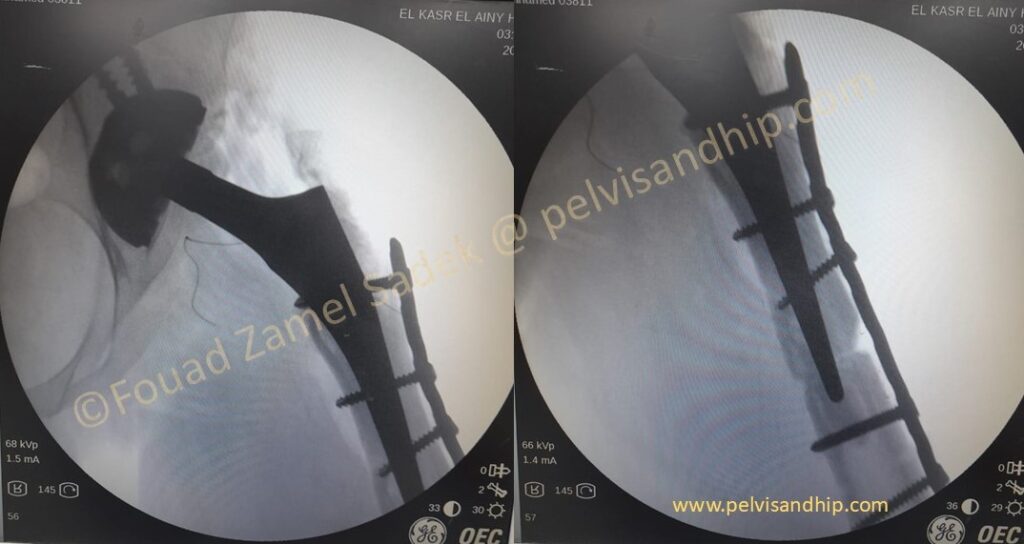
With the final rasp in situ, the transverse complete osteotomy was done at the level of the exit of the rasp top. The femur was aligned and after trial reduction an over riding segment from the distal femur was resected. Reduction and plate fixation was carried out with screws inserted avoiding the space for insertion of the definitive stem. Choice of either a cemented or a cementless stem fixation as at the surgeon’s discretion. In our case we opted for a cemented stem for soft bone condition.

The final picture with the completed reconstruction provided a well aligned stable construct with a balanced pelvis and corrected leg length.

Fixation of the osteotomy carefully carried out did not jeopardise a good cementing technique an essential part to ensure longevity
At 3 months follow up. Patient is walking full weight bearing with no support. The amount of union at the osteotomy site is quite reassuring.
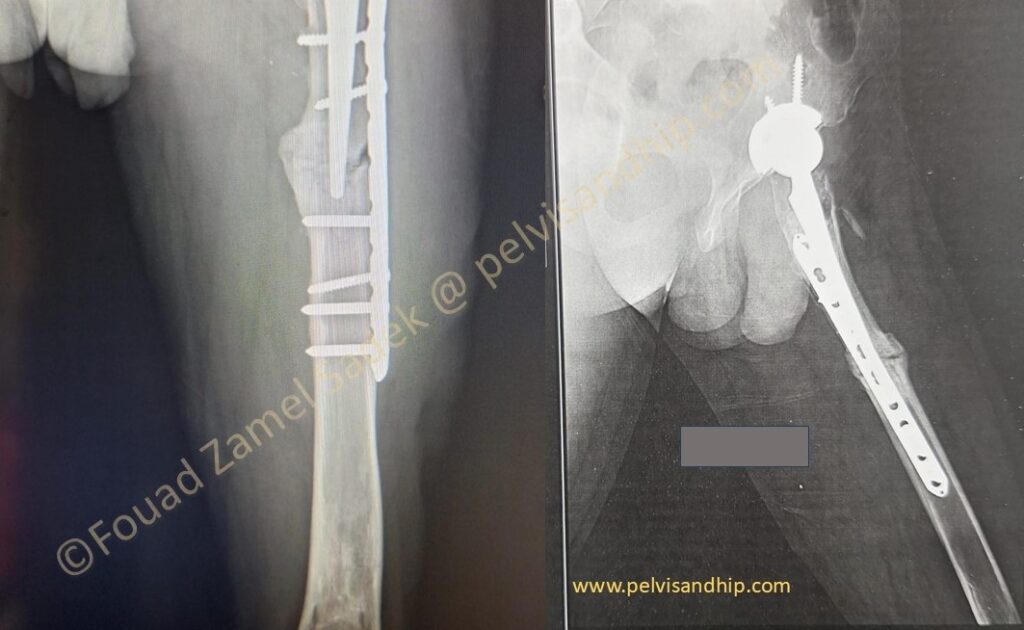
7 months after surgery patient is allowed to carry out all activities with no restrictions. The abundant callus formation is obvious with nearly complete healing of the femoral osteotomy.